SAN FRANCISCO – Tight glycemic control helps normalize thyroid hormone concentrations following cardiac surgery in children, according to results from a randomized trial presented at the Endocrine Society’s annual meeting.
That could be important because "it’s well known that cardiac surgical procedures can induce nonthyroidal illness in children" – a brief free-hormone surge followed by low T3 (triiodothyronine) and T4 (thyroxine) and increased rT3 (reverse triiodothyronine). It’s associated with longer recoveries, said lead investigator Dr. Carmen Soto-Rivera, an endocrinologist at Boston Children’s Hospital.
But it’s difficult to say what the clinical implications of her team’s findings are, she noted, because "we still don’t know if nonthyroidal illness is adaptive or maladaptive."
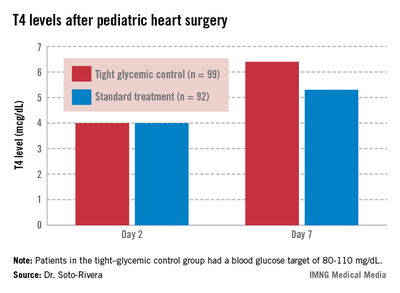
The study involved 191 children who underwent cardiac surgery with cardiopulmonary bypass. After surgery, her team randomized 99 children who were 0-36 months old to tight glycemic control, with a blood glucose target of 80-110 mg/dL; and 92 others to the standard treatment, permissive hyperglycemia; their median blood glucose hovered around 120 mg/dL.
Two days after surgery, 98% of the children had T4 and T3 levels below age-specific normal ranges, consistent with nonthyroidal illness. The thyroid hormone binding ratio (THBR) was normal in most of the patients, so it did not explain the drop in T4 and T3.
The groups had begun to separate by day 7. Tight-control patients had a higher median T4 than did patients on standard treatment (6.4 vs. 5.3 mcg/dL; P = .02) and a greater median T4 change from day 2 (2.4 vs. 1.3 mcg/dL, P = .02).
The trend continued among children still in the hospital on day 14. The 30 tight-control patients, compared with 37 on standard treatment, had a higher median T3 (104.5 vs. 74 ng/dL; P = .02) and a greater change from day 2 (26 vs. 5 ng/dL; P = .02). They had a higher T4 on day 14 too, but the difference was not significant.
"Interestingly, we found that [tight glucose control] resulted in lower [C-reactive protein] levels by day 7," about 3 mg/L, versus about 4 mg/L in the standard-treatment arm (P = .01). Perhaps "the faster increase in thyroid hormone levels may be mediated by decreased inhibition of deiodinases due to lowered inflammation," Dr. Soto-Rivera said.
The findings differ from previous reports of tight glucose control increasing peripheral inactivation of thyroid hormone, she said. "We believe that because our glucose targets were higher and we had [a low] rate of hypoglycemia in both arms, we potentially prevented a fasting response in these children," leading to decreased inhibition of the thyroid axis, she added.
"We believe that almost no one was treated with thyroid replacement during [the study], but we are in the process of confirming this," she said.
The project was a subgroup analysis of a larger trial that found no significant benefit for tight glycemic control on infection rates, mortality, length of stay, and organ failure following pediatric heart surgery (N. Engl. J. Med. 2012;367:1208-1219).
Dr. Soto-Rivera said she had no disclosures. The National Institutes of Health funded the project.