Mr. Brown is a physician assistant in the Urology Department at the VA Salt Lake City Health Care System in Utah and a lieutenant colonel in the Utah Air National Guard. Mr. Smith is an Emergency Department physician and a major in the Utah Air National Guard. Mr. Kirkland is a training manager and a master sergeant in the West Virginia National Guard.
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review the complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Mental status changes are usually described as fatigue, lethargy, disorientation, headache, seizure and coma. Indeed, mental status changes may be one of the most important factors that can assist the clinician in the identification, mitigation, and treatment of heat injury before it reaches a critical stage. Clinical familiarity with and diagnosis of delirium resulting from heat injury could prove beneficial in protecting an individual exposed to severe heat environments.
In 2011, Becker and Stewart suggested that in the absence of hyperthermia, the presence of central nervous system (CNS) symptoms should prompt the clinician to pursue another diagnosis.6 However, a core temperature of 104°F with associated CNS changes and anhydrosis should be defined as heat stroke and is a medical emergency.6
Death rates from excessive heat are documented as high as 31%.7 Signs of CNS dysfunction such as irritability, ataxia, headache, nausea, vomiting, anhydrosis, confusion, and decreased cognitive function are essential to the diagnosis of heat stroke. Classic heat stroke will present as a triad of hyperpyrexia, anhydrosis, and mental status changes.8 However, making the diagnosis of heat stroke based on anhydrosis could be dangerous, because in exertional heat stroke, many patients continue to sweat. Overlooking the diagnosis of heat stroke based on anhydrosis could lead to a delay in treatment and severe complications.8 These complications may include hyperkalemia, hyperphosphatemia, hypocalcemia, and myoglobinuria.
Once heat stroke has occurred, coagulopathies may manifest as epistaxis, and endothelial damage may present as peripheral or pulmonary edema. Additionally, a core temperature of above 104°F may trigger a cascade of events that may include systemic inflammatory response resulting in increased cell wall permeability and release of endotoxins. These events can lead to tissue hypoxia, metabolic acidosis, and organ failure. Sequalae from heat stroke can result in multisystem failure. A 1998 study of Chicago heat wave victims reported that the degree of functional disability predicted survival at 1 year.9 Although hospital mortality was 21%, severe functional impairment at discharge was 33%, with an additional 28% mortality at 1 year.9 And the 1-year mortality from heat stroke is similar to that of cerebral vascular accidents.10 Within 24 hours, heat stroke victims often will display evidence of muscle, kidney, and cardiac dysfunction. Delay in intervention raises the risk of fatalities associated with hyperthermia.11,12 Tissue destruction due to uncompensated heat may lead to rhabdomyolysis and subsequent myoglobinuria and renal injury. Damaged hepatocytes may lead to coagulopathies and hepatitis. Injured heart muscle may lead to arrhythmias and cardiac arrest.
The CNS symptoms may be difficult to ascertain in an intense working environment. The CNS system dysfunction is indicative of progression from heat injury to heat stroke and thus a medical emergency. It is imperative that the clinician be able to assess the individual quickly and accurately.
Delirium
Along with physical problems associated with it, heat injury can also lead to relatively abrupt mental status changes. In 2005, Glazer reported that even with minimally elevated core temperatures, CNS system changes can present with altered mental status, convulsions, and coma.13 This qualifies as a medical emergency known as delirium. Patients with delirium may present with a history of abrupt and fluctuating levels of consciousness. This fluctuation in symptoms that resemble sepsis could confuse medical providers.13 Thus, it is imperative that there be continuity of care of the patient with the ability to compare states of consciousness longitudinally over time.
In 1984, Pérez reported that nurses, perhaps because of their familiarity with and proximity to the patient, recorded delirium in 93% of patients, whereas psychiatric consultants recorded delirium only 34% of the time.14 Delirium manifests with several neurologic signs and symptoms; these include but are not limited to tremor, myoclonus, difficulty reading and writing, and visuoconstructive deficits, such as copying designs and problem solving.15 No matter the method to discover the delirium, the definitive treatment is to identify and treat the underlying medical condition.15 The CNS system dysfunction consistent with delirium such as irritability, ataxia, and confusion are essential to the diagnosis of heat stroke.13 Coma and seizures may occur, and retarded recovery of functional ability is an indication of a poor prognosis.9
Objective
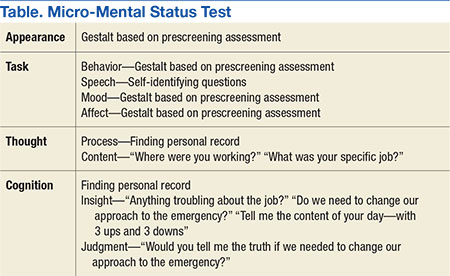
The authors propose that in addition to vital signs, an assessment of a patient’s mental status through the use of a mental status exam could be a tool that identifies the problem early and avoids the progression of symptoms from heat stress to heat exhaustion and heat stroke. Early intervention in the progression of symptoms of hyperthermia can save lives, decrease suffering, and maintain a more robust mission-ready posture for the individual and the unit.