Referrals
To address the problems with referrals that plague other CR programs, staff of the Healthy Heart Program worked closely with interventional cardiology and the cardiothoracic team, including the clinical informatics coordinators, to develop an automatic referral system for CR evaluation. Consults for CR evaluation were embedded within the post-CABG and PCI order sets in the electronic health record. Laboratory troponin alerts were created to alert CR staff of patients with elevated troponins, which identified patients admitted for acute MI. Healthy Heart Program staff members received the referrals once a patient was admitted to the unit following their heart procedure. Early referrals for evaluation allowed staff to begin a chart review of all eligible patients and to follow the patient’s course of recovery. Most consults were generated during hospitalization for one of the indications; however, a minority of consults come from both the cardiology and primary care clinics.
Three Phases of CR
The AACVPR describes the challenges and opportunities found throughout the CR continuum.5 Over the past several decades, the continuum of care was more program centered and service utilization was more isolated. Today, CR is viewed as more process oriented and coordinates care across many professionals and services. Phase 1 inpatient CR begins in the hospital and is a shared responsibility between several services. Shortened hospital stays have led to innovative solutions for early ambulation, risk factor education, and discharge planning, including enrollment into phase 2 CR. Phase 2, also known as early outpatient, should begin within 1 to 2 weeks postevent in healthier patients and can last between 6 and 12 weeks postdischarge. Phase 3 (maintenance phase) should begin immediately at the conclusion of phase 2.
Phase 1
Prior to the advent of the Healthy Heart Program, secondary prevention education was not done at the bedside for SFVAMC patients following cardiac revascularization. The AACVPR recommends patient assessment, mobilization, risk-factor identification and education, and facilitation into outpatient CR as essential components of phase 1 CR.5 The Healthy Heart Program clinician initiates phase 1 CR by examining cardiac risk factor management for all referred patients. Physical and cardiac risk factor assessments are accomplished by completing a detailed chart review and interview with the patient. During this interview with the patient, the clinician evaluates cognitive function and readiness to learn. Staff will interview the patient further to assess the overall patient needs, including availability of social support, resources to maintain optimal health, and the need for secondary preventive education. For the PCI patient, the interview may occur in the hours following their procedure; for the surgical patient, this bedside visit typically occurs postoperative day 3 or 4.
A standardized cardiac risk factor evaluation tool was designed, which also serves as an education form to help guide the conversation on risk factor management. The interactive, patient-centered form includes opportunities to review risk, discuss current laboratory values (eg, lipids and hemoglobin A1c), and establish individualized goals based on patient preference and recommended guidelines. Healthy Heart Program staff assist the patient in formulating achievable goals using the SMART (specific, measurable, attainable, realistic, and time-related) criteria.19 Immediately after a heart event or procedure, patients often feel highly motivated to initiate lifestyle changes.20 However, PCI patients may have a short window of opportunity for learning between their readiness to learn state and before the activities of discharge. Staff use these opportunities as a teachable moment and to increase enrollment into outpatient CR (phase 2).
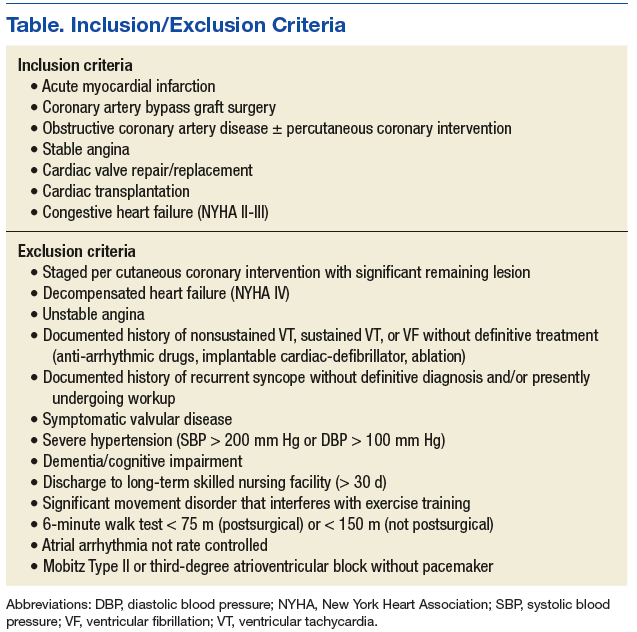
The provider performs a thorough chart review and bedside consultation to determine whether home-based CR is indicated, feasible, and appropriate. Not every patient that is referred will be enrolled in CR. Patients have the option to opt out. In addition, clinical staff adhere to the program protocol’s exclusion criteria.
Absolute contraindications for home enrollment include unstable angina, staged cardiac procedure (PCI and surgery), complex ventricular arrhythmias, severe or symptomatic aortic stenosis, decompensated heart failure, and uncontrolled hypertension (Table). Patients deemed high risk for home-based CR may be referred to a non-VA facility-based CR program. Risk stratification, using the Canadian Cardiovascular Society Grading of Angina Pectoris, is a continuous process that is used to identify patients who may move from moderate to high risk, both before and during the program.21,22
Phases 2 and 3
Phase 2 of the Healthy Heart Program CR includes physical activity, risk-factor modification, nutritional guidance, psychosocial modification, a return to previous activities, and an improved QOL. Prior to entry into the program, a submaximal exercise test, the 6-minute walk test (6MWT), is used as both a qualifying test and for developing the initial exercise prescription.22 The minimum 6MWT distance needed to qualify is 75 m for postoperative and 150 m for nonsurgical patients. The 6MWT is performed in-hospital for patients who were admitted for stable angina, PCI, and are > 4 days following acute MI.23 Cardiothoracic surgery patients are tested at their first follow-up clinic visit (typically 2-3 weeks postoperatively). The clinician monitors the heart rate with either a wearable device or via inpatient telemetry monitors. This exercise testing also serves as a motivational tool for patients to gain confidence in their ability to begin to exercise at home.