Susan Lava-Parmele is a Staff Physician, Rebecca Rudquist is a Research Study Coordinator, Janeen Trembley, Tammy Butterick, and Ronald Bach are Research Health Scientists, all at the Minneapolis Veterans Affairs Health Care System in Minnesota. Nicole Baldwin is a Medical Student; Janeen Trembley is an Adjunct Assistant Professor; Tammy Butterick is an Adjunct Assistant Professor, Department of Food Science and Nutrition and a Graduate Faculty Member in the College of Food, Agriculture and Nutrition; and Ronald Bach is an Associate Professor, all at the University of Minnesota in Minneapolis. Correspondence: Ronald R. Bach (ronald.bach@va.gov)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
To determine areas of GWI health care that needed QI at the MVAHCS, veterans with GWI were contacted for a telephone survey. These veterans had participated in the Gulf War Illness Inflammation Reduction Trial (ClinicalTrials.gov. Identifier: NCT02506192). Therefore, all met the Kansas case definition for GWI.4 The aim of the survey was to characterize veterans’ experiences seeking health care for chronic postdeployment symptoms.
Sixty Gulf War veterans were contacted by telephone and invited to participate in a 15-minute survey about their experience seeking diagnosis and treatment for GWI. They were informed that the survey was voluntary and confidential, that it was not part of the research trial in which they had been enrolled, and that their participation would not affect compensation received from VA. Verbal consent was requested, and 30 veterans agreed to participate in the survey.
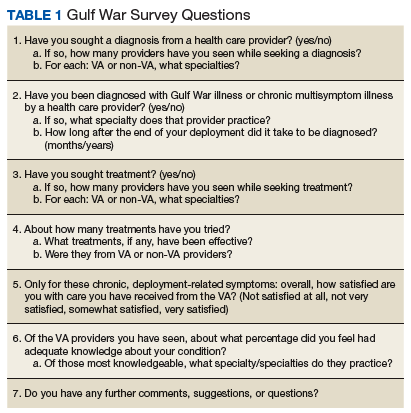
The survey included questions about the course of illness, disability and service connection status, HCPs seen, and suggestions for improvement in their care (Table 1).
Questions were designed to characterize each veteran’s experiences with GWI, the impact of symptoms, specialists who most often saw patients with GWI, perspectives about their care, and areas where they thought there was potential for improvement. The objective was to identify common difficulties and gaps in health care experienced by veterans as well as potential areas on which to focus improvement. The goal of this QI study was to translate survey results into recommendations that might improve the quality of medical care for veterans experiencing GWI.
Results
Of the 30 veterans who participated in the survey, most were male with only 2 female veterans. This proportion of female veterans (7%) is similar to the overall percentage of female veterans (6.7%) of the first Gulf War.2 Ages ranged from 46 to 66 years with a mean age of 53. Mean duration of illness, defined as time elapsed since perceived onset of chronic systemic symptoms during or after deployment, was 22.8 years, with a range of 4 to 27 years. Most respondents reported symptom onset within a few years after the end of the conflict, while a few reported the onset within weeks of arriving in the Kuwaiti theater of operations. A little more than half the respondents considered themselves disabled due to their symptoms, while one-third reported losing the ability to work due to symptoms. Respondents described needing to reduce hours, retire early, or stop working altogether because of their symptoms.
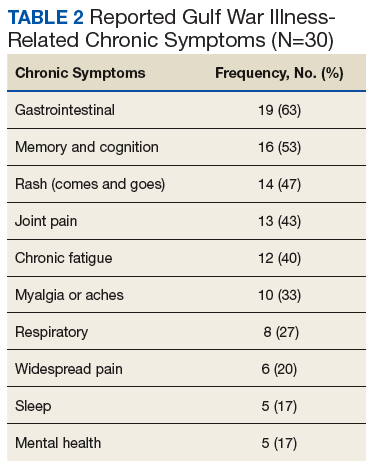
Respondents attributed several common chronic symptoms to deployment in the Gulf Wars (Table 2).
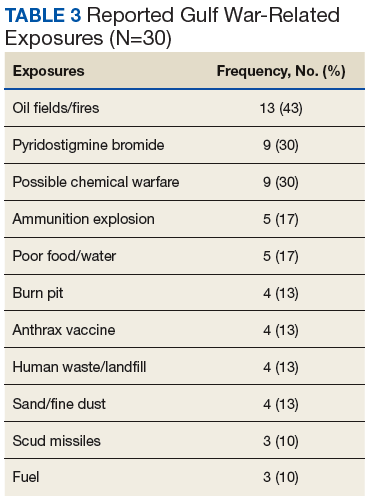
Notably, the top symptoms reported also were the 6 main symptom domains of the Kansas GWI cohort: fatigue/sleep problems, muscle/joint/body pain, neurologic/cognitive/mood symptoms, GI symptoms, respiratory symptoms, and skin symptoms, with sinus congestion the most common among “other symptoms.”4 A few veterans commented that their friends who were Gulf War veterans struggled with the same symptoms as they did. Respondents also were questioned about environmental exposures during their Gulf War deployment without being prompted or given examples (Table 3).
Their responses were representative of common exposures cited in other studies,providing further support that their experiences were comparable with those of veterans in other GWI studies.14
Most veterans surveyed were service connected for individual chronic symptoms. Some were service connected for systemic conditions such as fibromyalgia (FM), chronic fatigue syndrome (CFS), and irritable bowel syndrome (IBS) (5 veterans were connected for each condition). Three of the 30 veterans had been diagnosed with GWI—2 by past VA physicians and 1 by a physician at a GWI research center in another state. Of those 3, only 1 was service connected for the condition. Three respondents were not service connected at all.
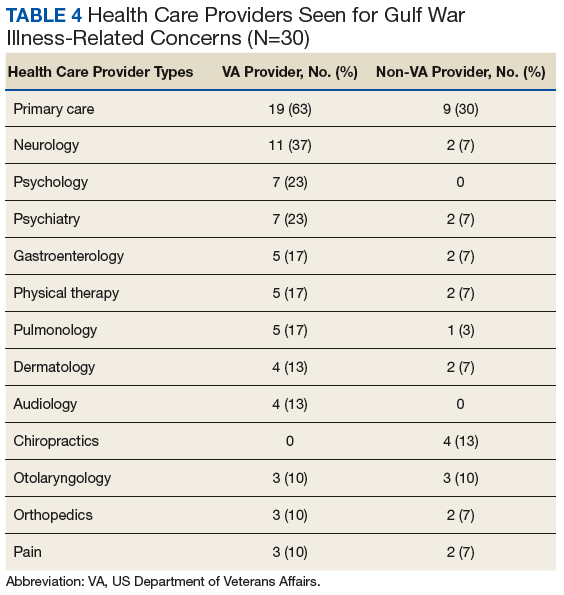
The most common VA HCPs seen were in primary care and neurology followed by psychiatry and psychology. Of non-VA HCPs, most respondents saw primary care providers (PCPs) followed by chiropractors (Table 4).
Before taking the Gulf War survey, a broad subjective question was posed. Respondents were asked whether VA HCPs were “supportive as you sought care for chronic postdeployment symptoms.” A majority of veterans reported that their VA HCPs were supportive. Reasons veterans gave for VA HCPs lack of support included feeling that HCPs did not believe them or trust their reported symptoms; did not care about their symptoms; refused to attribute their symptoms to Gulf War deployment; attributed symptoms to mental health issues; focused on doing things a certain way; or did not have the tools or information necessary to help.
Most non-VA HCPs were supportive. Reasons community HCPs were not supportive included “not looking at the whole picture,” not knowing veteran issues, not feeling comfortable with GWI, or not having much they could do.
Veterans were then asked whether they felt their HCPs were knowledgeable about GWI, and 13 respondents reported that their HCP was knowledgeable. Reasons respondents felt VA HCPs were not knowledgeable included denying that GWI exists, attributing symptoms to other conditions, not being aware of or familiar with GWI, needing education from the veteran, avoiding discussion about GWI or not caring to learn, or not knowing the latest research evidence to talk about GWI with authority. Compared with VA HCPs, veterans found community HCPs about half as likely to be knowledgeable about GWI. Many reported that community HCPs had not heard of GWI or had no knowledge about it.
Respondents also were asked what types of treatments they tried in order to typify the care received. The most common responses were pain medications, symptom-specific treatments, or “just putting up with it” (no treatment). Many patients were also self-medicating, trying lifestyle changes, or seeking alternative therapies.
Finally, respondents were asked on a scale of 0 (very unsatisfied) to 5 (very satisfied), how satisfied they were with their overall care at the VA. The majority were satisfied with their overall care, with two-thirds very satisfied (5 of 5) or pretty satisfied (4 of 5). Only 3 (10%) were unsatisfied or very unsatisfied. Respondents had the following comments about their care: “They treat me like I am important;” “I am very thankful even though they cannot figure it out;” “They are doing the best they can with no answers and not enough help;” “[I know] it is still a work in progress.” A number of respondents were satisfied with some HCPs or care for some but not all of their symptoms. Reasons respondents were less satisfied included desiring answers, feeling they were not respected, or feeling that their concerns were not addressed.
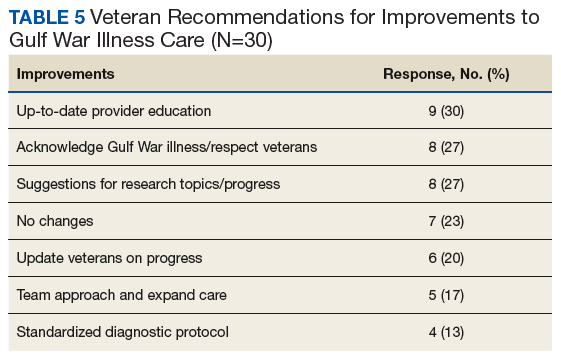
When asked for suggestions for improvement of GWI care, the most common response was providing up-to-date HCP education (Table 5).
One veteran suggested that information provided annually by the National Research Advisory Council about GWI research updates should be made available to HCPs as an accessible summary. Respondents also wanted to ensure that they were respected for their service and that HCPs are taught to acknowledge and ask about GWI symptoms, especially for Gulf War veterans. Another common suggestion was to provide regular updates to the veteran community about research progress. A number were concerned that GWI and the exposures involved were “being treated like Agent Orange” with respect to the slow progress and dissemination of research. Others specifically requested an interdisciplinary team approach for veterans who may have GWI, such as a specialty clinic or center of excellence. Other requested changes in care included greater flexibility within VAHCS such as expanding ability to get coverage outside VAHCS and creating a way to obtain service connection for GWI. Finally, 2 respondents specifically requested that HCPs adopt a standardized diagnostic protocol.