News

AGS issues pandemic resource allocation recommendations amid ageism concerns
Rationing strategies that are solely, or predominantly, based on age cutoffs could lead to persistent beliefs that older adults’ lives are less...
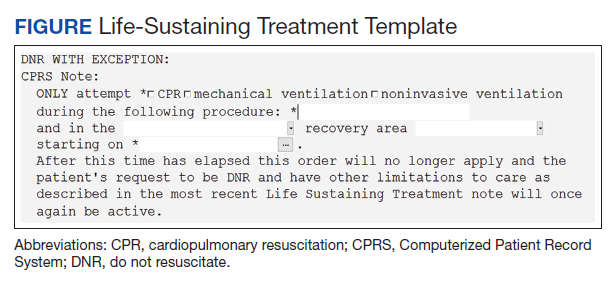
Background: In 2017, the US Department of Veterans Affairs (VA) implemented the Life-Sustaining Treatment Decisions Initiative (LSTDI), which created a portable and durable code status for use across its health care system. Patients who now have a durable do not resuscitate (DNR) status may undergo invasive procedures. Few studies have examined whether proceduralists discuss DNR status and document changes before procedures.
Objective: To assess baseline percentage of suspension of DNR before nonsurgical invasive procedures and determine whether an academic detailing intervention consisting of training proceduralists in the use of a template that allows rapid suspension of DNR status increases percentage of DNR acknowledgments.
Methods: Single-center, quasi-experimental pre- and postassessments were done in high-volume, procedural areas, including gastroenterology, cardiology, and interventional radiology, in a VA medical center. The primary outcome was the proceduralists’ documentation of DNR status acknowledgment before a nonsurgical invasive procedure at baseline and after the intervention. Logistic regression was used to compare percentage of DNR acknowledgment with time (before, after) and procedural area and assessing their interaction in the model.
Results: The interaction between department and time revealed wide variation in documentation of DNR acknowledgment. Examining the model predicted percentages from the interaction, preintervention percentages for gastroenterology, cardiology and interventional radiology were 46%, 75.6%, and 7.5%, respectively, and postintervention model predicted percentages were 53.5%, 91.7%, and 26.3%, respectively. Only the before vs after contrast for interventional radiology was significantly different. When all procedural areas were combined, the percentage of DNR acknowledgment significantly improved from 38.6% to 61.1% ( P = .01).
Conclusions: Before nonsurgical invasive procedures, the percentage of DNR acknowledgment was low but after, the intervention significantly improved. Further research is needed to assess its impact on patient-centered outcomes.
Rationing strategies that are solely, or predominantly, based on age cutoffs could lead to persistent beliefs that older adults’ lives are less...
A 99-year-old veteran, his family, and an anesthesiologist practice shared decision making to ensure patient-centered care before a procedure.