Dr. Sipes is a palliative care nurse practitioner in the Department of Geriatrics and Extended Care at the VA Northern Indiana Health Care System in Marion, Indiana. Dr. Siela is an associate professor of nursing at Ball State University in Muncie, Indiana. Dr. Rogers is the clinical pharmacy coordinator for the VA Northern Indiana Health Care System.
The primary aim of this quality improvement (QI) project was to educate the PCP about the importance of allowing veterans to express their care goals in the form of ADs and to understand that veterans would prefer to discuss these goals with their PCP. A secondary aim was to improve goal-directed care for veterans with COPD or CHF by increasing the number of completed ADs.
By using a systems approach, ACP can be addressed in a uniform manner. This approach allows veterans to discuss their goals of care prior to the need for emergent interventions, avoiding burdensome and unwanted treatments. Through the completion of ADs, veterans are able to designate a surrogate decision maker and identify specific desired treatments and interventions as their illness advances.
Two physicians and 3 nurse practitioners volunteered to contribute to this study. In the participating clinics, veterans with a diagnosis of CHF or COPD were identified. Each veteran had 20 to 30 minutes per appointment to discuss concerns, be examined, have HCPs address concerns, and complete all clinical reminders.
The study design was a QI project focused on evaluating the following process: An EMR reminder alerted the clinic nurse who asked the veteran if he or she was interested in completing an AD. If the patient agreed, a consult was placed to the social worker for completion of the VA national form for AD. The completion rate for a sample of primary care clinics at the facility was 10% to 12%, with no participation from the PCP in the process.
The providers were educated in 5 areas: (1) the prevalence of CHF and COPD in the U.S.; (2) the difference between ACP and AD; (3) the percentage of ADs completed in the U.S. adult population and in the facility; (4) the importance of addressing ACP early in the disease trajectory of this population; and (5) the use of the EMR reminder and the template to guide discussion of ACP ( eAppendix A
The template was developed following the literature review and addressed the reoccurring themes that patients wanted to discuss concerning their specific diagnosis and treatment. The template was formatted to include 3 components: (1) health care surrogate; (2) code status; and (3) organ donation preference ( eAppendix B
). When EMR reminders appear, the PCP initiated a discussion regarding COPD or CHF and the likely progression of the illness. The provider opened a separate note entitled AD Discussion and uses the template. The provider could then guide the discussion to the veteran’s goals of care.
The natural progression from discussion of goals of care led to the discussion regarding the initiation of an AD. When completed, the note automatically appeared in the Postings section of the EMR, making it easily accessible to all other providers in different care settings.
The project time was 3 months (December 2012 through February 2013). The education was completed and the EMR reminder was turned on at the beginning of the project for veterans with a diagnosis of CHF or COPD who had not completed an AD. At the conclusion of the project, the PCPs completed a post project survey to provide information regarding their opinions on facilitators and barriers in the AD completion process ( eAppendix C
). The intervention of the PCP-initiated discussion of ACP was assessed by the percentage increase in completed ADs.
Results
Five different primary care clinics in 4 different locations throughout the health care system provided a total of 294 veterans with diagnoses of CHF or COPD. On completion of the project, 35 veterans had completed ADs. These 35 veterans represent an additional 12% of patients who previously did not complete an AD despite being approached multiple times. The veterans completed an AD following PCP-initiated discussion due to this QI project.
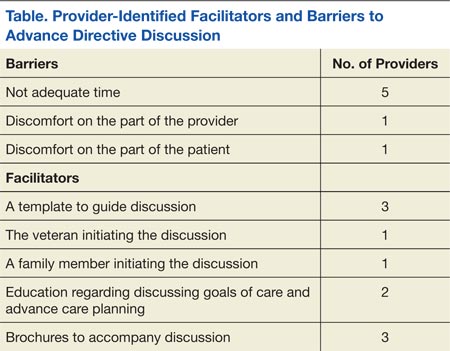
All 5 providers completed the post project survey and agreed that it would be beneficial to have the information regarding ADs easily accessible in the EMR. Four out of 5 providers admitted to cutting corners by not opening a new note every time to complete the AD template. They reported completing the EMR reminder within the clinic note, making it difficult to locate the information. Providers also reported on the various facilitators and barriers to AD discussion with patients (Table).
Discussion
The completion of an AD remains an important part of health care that is often neglected. When patients receive care and treatments, they often do not desire an AD, because the goals of care have not been clearly communicated and clearly documented. This can lead to poor quality of care with increased dissatisfaction and burden on the patient and health care system.14 However, if goals of care are discussed and documented, the veteran may avoid these burdensome treatments, and health care will be congruent with patient wishes. Better communication and documentation promotes increased patient satisfaction and improved quality of health care.1