Related: Prevention of Venous Thromboembolism After Total Joint Replacement: Rivaroxaban Update
This analysis emphasizes pharmacologic thromboprophylaxis instead of the combined endpoint of pharmacologic plus nonpharmacologic thromboprophylaxis traditionally used and will supplement the limited literature in 2 understudied cohorts: (1) nonsurgical veteran patients, specifically where advanced computerized thromboprophylaxis alerts are not in use; and (2) patients with the VTE risk factor of respiratory disease.1,7-9,12,13,15,16,18,21
Study Design
This observational study used retrospectively collected data. The data were extracted electronically from the VISN 9 data warehouse by a Decision Support Services analyst and manually validated by an investigator using the CPRS. Prior to initiation of research activities, the VHA Institutional Review Board and the Research and Development Committee at the facility level approved the study.
Sampling
Patients assigned to the treating specialties of medicine and medical critical care during fiscal years 2006 to 2008, admitted for ≥ 24 hours, and discharged with a diagnosis of chronic obstructive pulmonary disease (COPD), asthma, or acute, severe respiratory disease (eg, patients requiring mechanical ventilation) were eligible for inclusion. The authors also elected to include patients with asthma, because this diagnosis commonly overlaps with COPD and reflects real-world clinical practice and diagnostic challenges.28 Pneumonia and other infectious pulmonary conditions were not a qualifying diagnosis for study inclusion.
Patients were excluded if aged > 79 years, because it is difficult to maintain de-identification in a small sample of inpatients in this age category. Unfortunately, octogenarians have the highest rate of VTE per 100,000 population and would gain substantial benefit from prophylaxis.29 Similar to other VHA and non-VHA investigators, this study excluded patients who were prescribed therapeutic anticoagulation.7,12,21,30 The authors believe continuation of therapeutic (or treatment) anticoagulation does not measure a clinical decision to use pharmacologic thromboprophylaxis, and any interruption of therapeutic anticoagulation suggests that prophylactic anticoagulation is not warranted.
Related: Pulmonary Vein Thrombosis Associated With Metastatic Carcinoma
Additionally, patients were excluded if length of stay (LOS) exceeded 14 days, if known or potential contraindications to thromboprophylaxis existed, or if laboratory data that were needed to assess for contraindications were missing from the electronic data set. Known or potential contraindications included active hemorrhage, hemorrhage within the past 3 months, recent administration of packed red blood cells, bacterial endocarditis, known coagulopathy, recent or current heparin-induced thrombocytopenia, or a potential coagulopathy (International Normalized Ratio > 1.5, platelets < 50,000, or an activated partial thromboplastin time > 41 sec).
Contraindications were conservative in construct and were similar to the exclusion-based VTE checklist for the nonsurgical patient.31 The authors did not examine the electronic data set for the contraindication of epidural or spinal anesthesia, because neither is commonly used in the medical ward or medical CCU. The authors also did not exclude patients with a creatinine clearance (CrCl) < 10 mL/min (a relative contraindication to VTE thromboprophylaxis), although these patients may be at an increased risk for bleeding complications.32
Endpoints and Measures
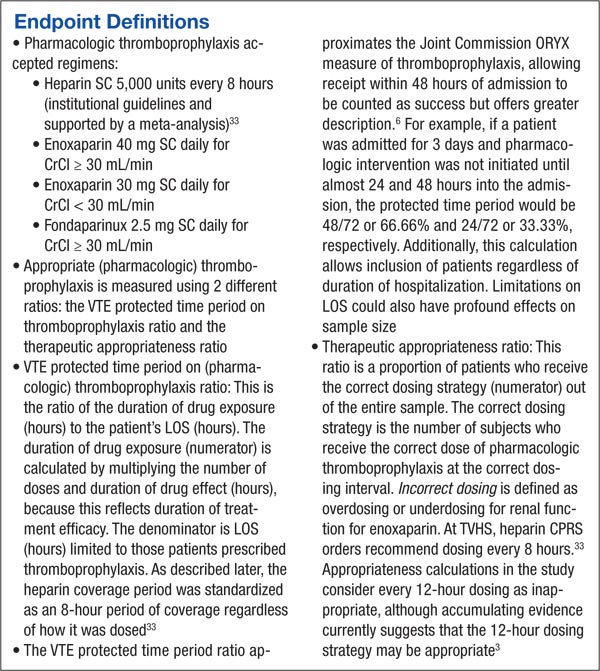
The primary endpoint of this study was the rate of any pharmacologic thromboprophylaxis (eg, ≥ 1 doses), similar to the endpoint selected by other investigators.7-9,12,13,15,16 Secondary endpoints included VTE protected time period on thromboprophylaxis, therapeutic appropriateness ratio for heparin and enoxaparin doses combined, and pharmacologic thromboprophylaxis rates according to level and location of care.
Sample Size
Although data have been forthcoming, at the time of study inception no studies documented the rate of pharmacologic thromboprophylaxis alone (defined as use of ≥ 1 dose of a pharmacologic agent) in patients with the VTE risk factor of respiratory disease.15,23 However, an average combined pharmacologic and nonpharmacologic thromboprophylaxis rate of 48.8% was determined from available studies.11,14 Although this percentage is an overestimate of pharmacologic thromboprophylaxis rates alone, this value was used to determine a sample size for the cohort.
About 122 subjects would be needed to provide 80% power and a significance level of < 0.05 to assess the hypothesis that pharmacologic prophylaxis rates at TVHS would exceed 60%. Additionally calculated was the sample size necessary to find a 20% expected difference in thromboprophylaxis rates according to location of care (eg, medical ward vs medical CCU), the secondary endpoint. This sample size was calculated to be 180 subjects, or 90 patients in each arm, to provide 80% power and a significance level (2-tailed alpha) of < 0.05. Subsequently, up to 130 patients from each location of care were randomly selected for study inclusion.
Data Analysis
A chi square test was used to compare groups on categorical variables. SPSS version 16.0 (SPSS Chicago, IL) was used for data analysis.
Results
A sample of 3,762 hospitalizations for veterans with COPD, asthma, or acute, severe respiratory disease who received inpatient care in the medical ward or medical CCU were extracted from the data warehouse.