Yeun-Hee Anna Park is Chief of Hematology/Oncology; Alison Keller is a Research Coordinator; and Ta-Chueh Melody Hsu is a Research Nurse Practitioner, all at James J. Peters Veterans Affairs Medical Center, Bronx, New York. Balmatee Bidassie is an Industrial Engineer VA Center for Applied Systems Engineering (VA-CASE), VISN11 - Veterans Engineering Resource Center (VERC) at Richard L. Roudebush Veterans Affairs Medical Center, Indianapolis, Indiana. Vickie Venne was a Senior Genetic Counselor for the US Department of Veterans Affairs (VA) Genomic Medicine Services, and Sarah Colonna is a Hematologist/Oncologist; both at George E. Wahlen Veterans Affairs Medical Center, Salt Lake City, Utah. Douglas Hawley is a Hematologist/Oncologist at Cincinnati Veterans Affairs Medical Center, Cincinnati, Ohio. Lori Hoffman-Högg is a ONS Clinical Nurse Advisor for the Oncology Field Advisory Committee and VHA National Program Manager for Prevention Policy at Veterans Health Administration (VHA) National Center for Health Promotion and Disease Prevention, Durham, North Carolina and VHA Office of Nursing Services, Washington, DC. Bernadette Heron is a Program Manager at Veterans Health Administration, Pharmacy Benefits Management Services in Hines, Illinois. Anita Aggarwal is a Hematologist/Oncologist Washington Veterans Affairs Medical Center, Washington, DC.
A high-risk breast cancer screening questionnaire based on the Gail BCRAT and including lifestyle questions was developed and included as a note template in the VA EMR. The James J. Peters VA Medical Center, Bronx, NY (JJPVAMC) and the Washington DC VA Medical Center (DCVAMC) ran a pilot study between 2015 and 2018 using this breast cancer screening questionnaire to collect data from women veterans. Quality Executive Committee and institutional review board approvals were granted respectively.
Eligibility criteria included women aged ≥ 35 years with no personal history of breast cancer. Most patients were self-referred, but participants also were recruited during VA Breast Cancer Awareness month events, health fairs, or at informational tables in the hospital lobbies. After completing the 20 multiple choice questionnaire with a study team member, either in person or over the phone, a 5-year and lifetime risk of invasive breast cancer was calculated using the Gail BCRAT. A woman is considered high risk and eligible for chemoprevention if her 5-year risk is > 1.66% or her lifetime risk is ≥ 20%. Eligibility for genetic counseling is based on the Breast Cancer Referral Screening Tool, which includes a personal or family history of breast or ovarian cancer and Jewish ancestry.
All patients were notified of their average or high risk status by a clinician. Those who were deemed to be average risk received a follow-up letter in the mail with instructions (eg, to follow-up with a yearly mammogram). Those who were deemed to be high risk for developing breast cancer were asked to come in for an appointment with the study principal investigator (a VA oncologist/breast cancer specialist) to discuss prevention options, further screening, or referrals to genetic counseling. Depending on a patient’s other health factors, a woman at high risk for developing breast cancer also may be a candidate for chemoprevention with tamoxifen, raloxifene, exemestane, anastrozole, or letrozole.
Data on the participant’s lifestyle, including exercise, diet, and smoking, were evaluated to determine whether these factors had an impact on risk status.
Results
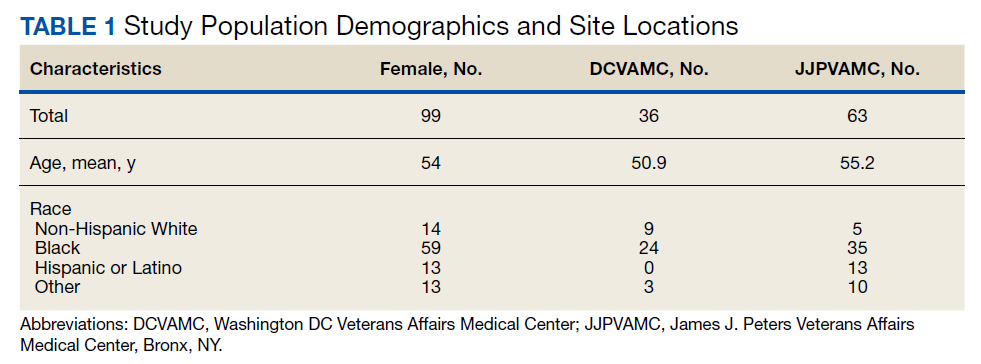
The JJP and DC VAMCs screened 103 women veterans between 2015 and 2018. Four patients were excluded for nonveteran (spousal) status, leaving 99 women veterans with a mean age of 54 years. The most common self-reported races were Black (60%), non-Hispanic White (14%), and Hispanic or Latino (13%) (Table 1).
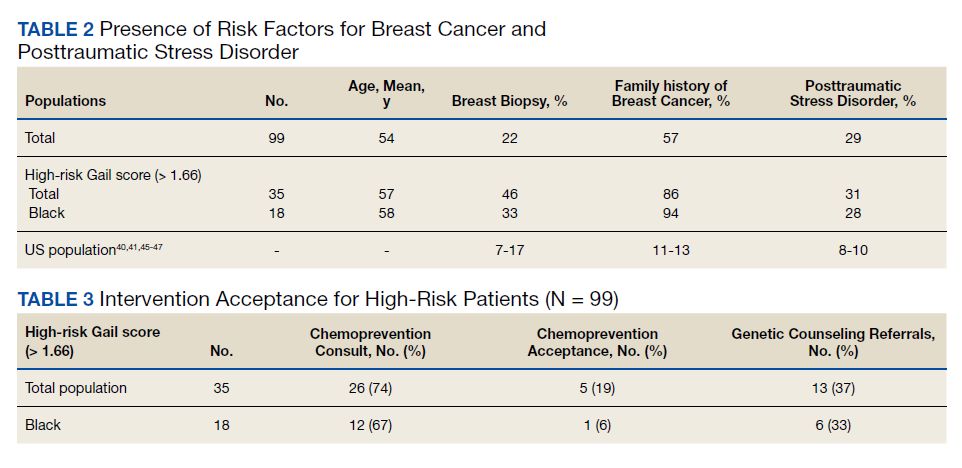
Women veterans in our study were nearly 3-times more likely than the general population were to receive a high-risk Gail Score/BCRAT (35% vs 13%, respectively).50,51 Of this subset, 46% had breast biopsies, and 86% had a positive family history. Thirty-one percent of Black women in our study were high risk, while nationally, 8.2 to 13.3% of Black women aged 50 to 59 years are considered high risk.50,51 Of the Black high-risk group with a high Gail/BCRAT score, 94% had a positive family history, and 33% had a history of breast biopsy (Table 2).
Of the 35 high-risk patients 26 (74%) patients accepted consultations for chemoprevention and 5 (19%) started chemoprevention. Of this high-risk group, 13 (37%) patients were referred for genetic counseling (Table 3).44 The prevalence of PTSD was present in 31% of high-risk women and 29% of the cohort (Figure).The lifestyle questions indicated that, among all participants, 79% had an overweight or obese body mass index; 58% exercised weekly; 51% consumed alcohol; 14% were smokers; and 21% consumed 3 to 4 servings of fruits/vegetables daily.