Early Parkinsonism: Distinguishing Idiopathic Parkinson’s Disease from Other Syndromes
Journal of Clinical Outcomes Management. 2015 June;22(6)
References
This review will discuss the most common presenting signs and symptoms of early IPD, present the most widely used diagnostic criteria, and introduce the ancillary laboratory and imaging tests that may be helpful in distinguishing it from its mimics. The diseases most commonly confused with early IPD will also be discussed with an emphasis on the ways they most commonly differ from IPD. We will begin our discussion with the presenting signs and symptoms of IPD.
Idiopathic Parkinson’s Disease
IPD typically has a subtle and insidious onset with characteristic features developing over months to years. IPD most often presents in patients after age 60, and age is the most consistent risk factor for developing IPD; however, approximately 5% of IPD cases begin before age 40 years. These young-onset cases are likely to be caused by genetic mutations [6]. The widely recognized cardinal motor features of IPD include asymmetric resting tremor, rigidity, bradykinesia and postural instability [7]. Asymmetry is a key feature, as symptoms typically start on one side and remain more prominent on that side as the disease progresses. In fact, lack of asymmetry suggests an alternative diagnosis. Of the cardinal motor features, tremor is most often reported by patients as the first symptom [8]. However, IPD can alternately present with various other motor or even nonmotor complaints that will be discussed later.
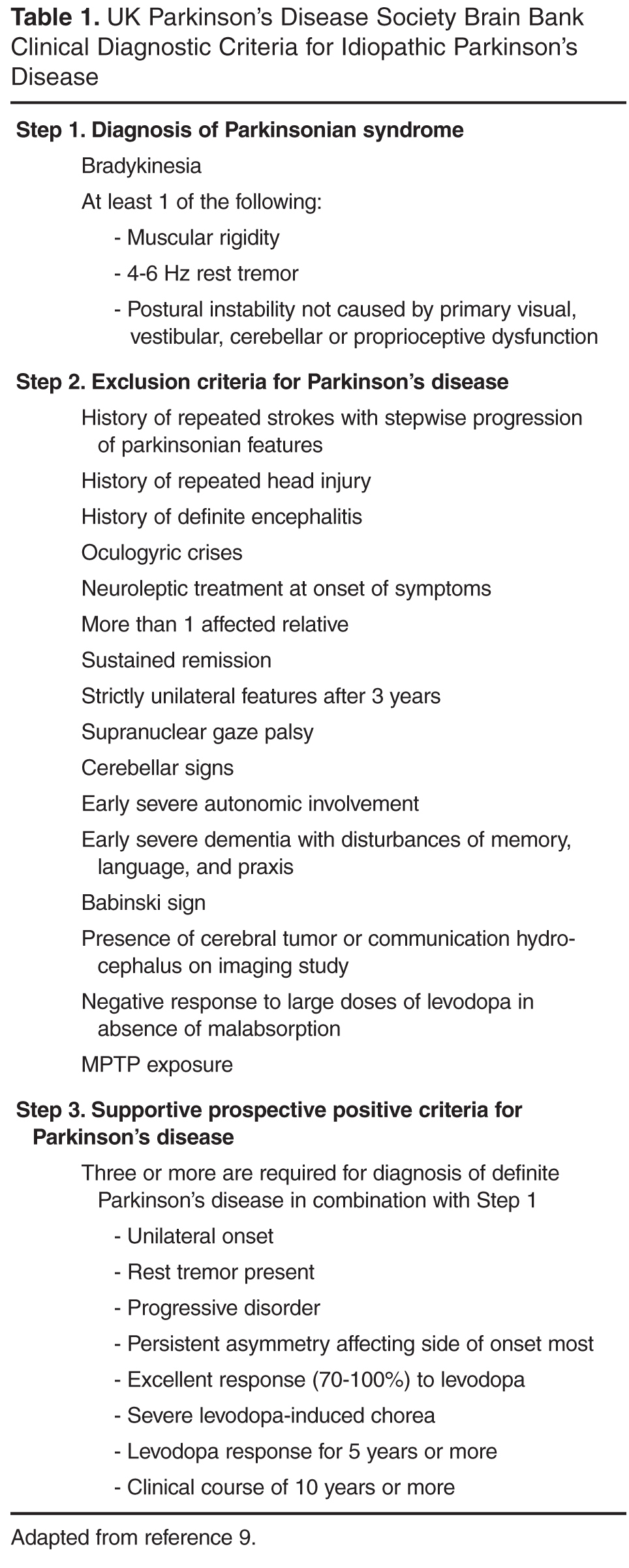
As stated previously, only the clinician can make the diagnosis. Ancillary tests are more often utilized to exclude other disease etiologies rather than to make the actual diagnosis of IPD itself. Brain imaging with MRI or CT is generally unremarkable but can sometimes be useful in ruling out other conditions in atypical cases. While genetic tests for the known causative genetic mutations are commercially available, they are never required for diagnosis and do not significantly alter the management approach. They are, therefore, most commonly reserved for the purposes of genetic counseling in individuals with a strong family history of PD. The UK Parkinson’s Disease Society Brain Bank clinical criteria are the most widely used diagnostic criteria for IPD and are featured in Table 1 . Despite the use of clinical criteria, the diagnostic certainty is still only between 75% and 90% when compared to autopsy results [9,10].
Motor Features
Resting tremor is the most common presenting sign/symptom of early IPD, found in approximately 70% of patients [8]. The tremor typically is asymmetric and intermittent at onset, often starting in one hand. It is sometimes, though not necessarily, described as a “pill-rolling” rhythmic movement of the thumb and first finger while the hand is at rest. Patients will usually report a worsening of tremor with stress, anxiety, and increased fatigue. The tremor does not persist during sleep and diminishes with voluntary activity of the affected limb(s). By having the patient perform mentally challenging tasks (such as counting backwards) or motor movements of other body parts (such as finger tapping with the other hand or walking), the examiner may notice an increase in tremor amplitude [11]. There may also be a resting tremor of the lip or lower jaw, but true head tremor suggests an alternate diagnosis such as essential tremor [12]. Postural tremor can co-exist with resting tremor in IPD, which often leads to diagnostic confusion, especially when the postural tremor is more prominent than the resting tremor. In this scenario, the distinction between IPD and essential tremor (discussed later) can become more difficult.