Following CDAD diagnosis, more than half of the study patients were isolated for 1 or more days. While the majority of patients with CDAD (74.0%) stayed in a general hospital room, 12.4% stayed in the ICU for a mean duration of 12.1 (± 12.3) days ( Table 3 ). Half of these ICU patients required
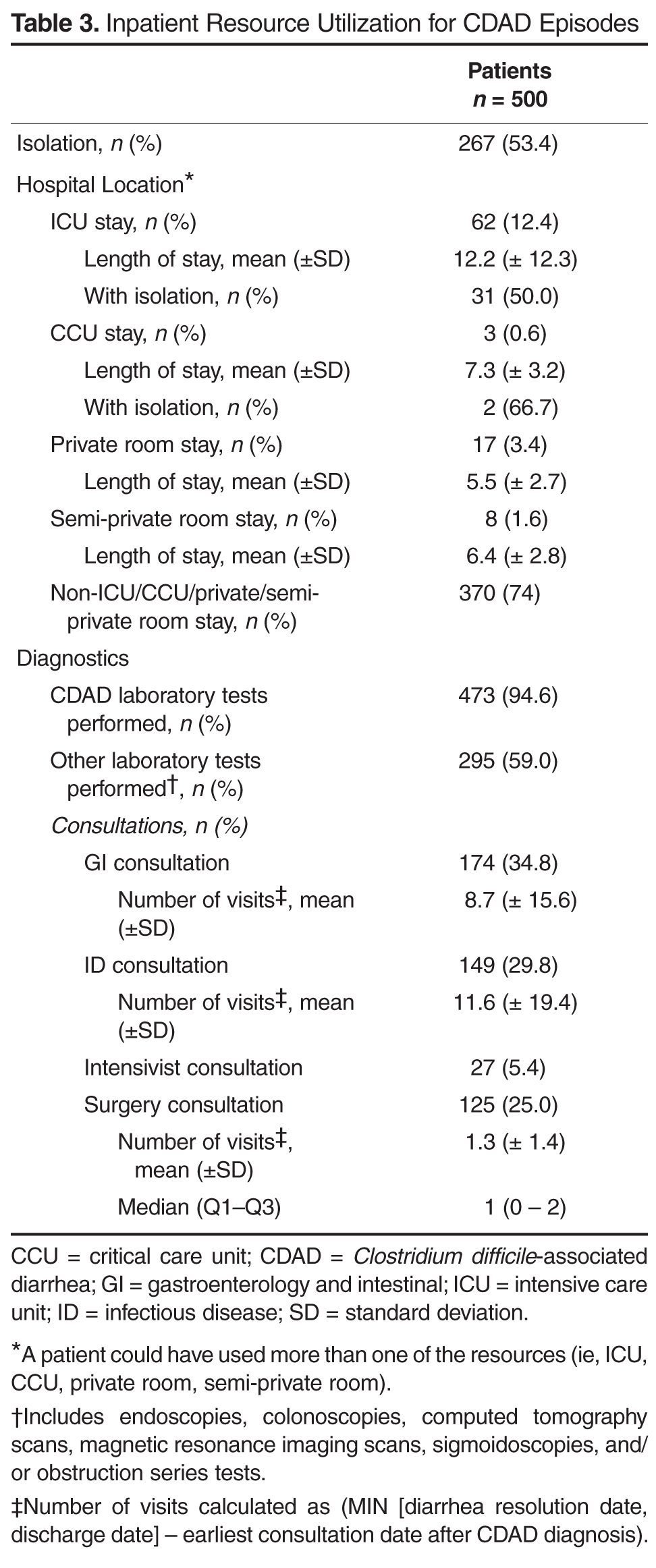
About one-third of patients consulted a gastrointestinal or infectious disease specialist at least once. Among these patients, assuming that a patient following an initial specialist consultation would have follow-up visits at least once a day (formal or informal) for the remainder of the CDAD episode, we estimate that there were an average of 8.7 (± 15.6) and 11.6 (± 19.4) GI or ID specialist visits respectively during the CDAD episode.
Nearly all patients had their CDAD diagnosis confirmed by laboratory tests. CDAD virulence was identified as toxin A and/or toxin B in 47.6% of the samples. However, nearly three-fifths of patients also underwent 1 or more nondiagnostic tests including endoscopy, colonoscopy, computed axial tomography (CAT), or magnetic resonance imaging (MRI) scans, sigmoidoscopy, and/or other obstructive series tests during the CDAD episode.
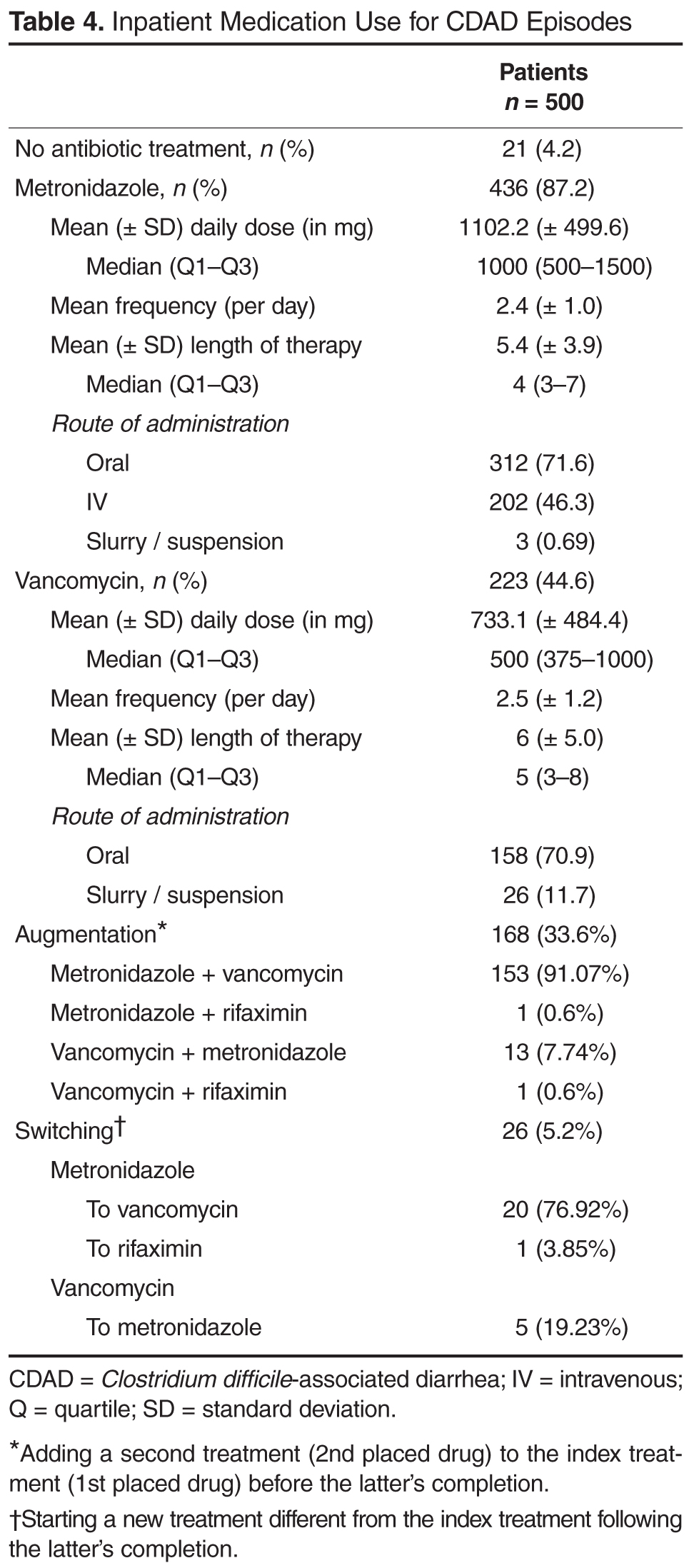
CDAD Treatment
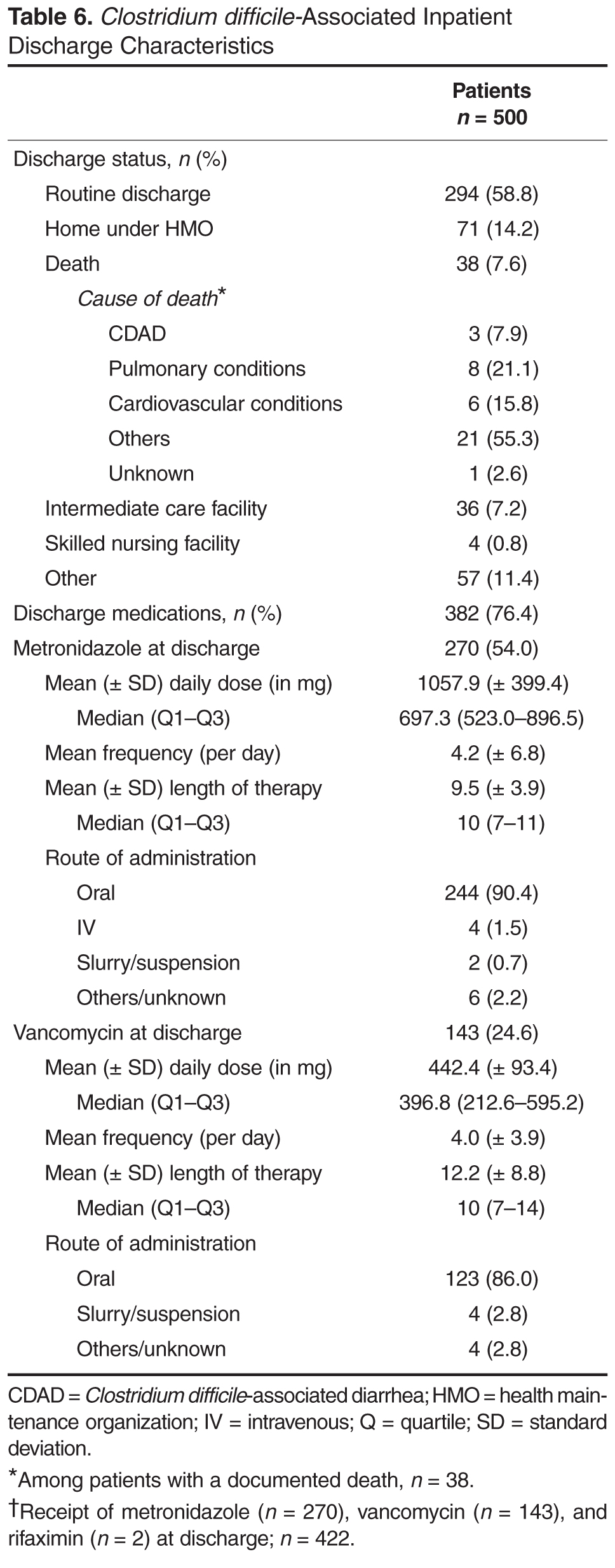
CDAD at Discharge
Hospitalization Costs
Based on claims data, the mean (±SD) and median (Q1–Q3) plan costs for the duration of a CDAD-associated hospitalization (2011 USD) for these 500 patients were found to be $35,621 (± $100,502) and $13,153 ($8,209–$26,893), respectively.
 Discussion
Discussion
While multiple studies have documented the considerable economic burden associated with CDAD [5–10], this study was the first to our knowledge to evaluate the specific hospital resources that are used during an extended hospital stay for CDAD. This real-world analysis, in conjunction with the Quimbo et al claims analysis, demonstrated the significant burden associated with CDAD in terms of both fixed costs (eg, hospital stay) as well as the variable components that drive these expenditures (eg, consultations, ICU stay).