Information Disclosure
One of the key areas impacted by culture relates to preferred disclosure of medical information. Walsh et al noted in their review that the majority of patients in English-speaking countries wanted relatively full disclosure regarding their illness in comparison to individuals from other countries [18].As a further distinction, Blackhall et al noted that African Americans and European Americans were more likely to believe that a patient should be told of a terminal diagnosis than Mexican and Korean Americans [19].In addition, Mexican and Korean Americans were more likely to believe that clinicians should not discuss death and dying with patients, as it could be harmful. Fujimori noted that Asians are less likely to prefer discussions of life expectancy in contrast to Westerners [20].In a survey of Albanian nationals, < 50% of patients wanted to know their true diagnosis; however, individuals who were male, urban, and educated demonstrated a significantly greater preference for disclosure [21].In the Middle East, the concept of disclosure is highly variable in terms of both provider and patient preferences [22].
Involvement of Family Members
A second important area relates to the involvement of family members. Fujimori noted high variability of patient preferences for having family members present when discussing bad news. Of Japanese patients, 78% preferred to be told with family members present, with the number decreasing for Portugal (61%), Australia (53%-57%), and Ireland (40%). Eighty-one percent of the US patients did not want anyone else present. However, almost all placed high value on physician expertise and honesty [20]. Blackhall noted that Mexican and Korean Americans were more likely to favor a family-centered approach to decision making [19]. In addition, Orona indicated that Mexican-American and Chinese-American families felt it was their duty to protect their relatives from a cancer diagnosis to keep the patient’s remaining time free of worry [23]. Haggerty found mixed evidence for patient preferences regarding disclosure of cancer prognosis to family members [24].
Given these variations and complexities, it is natural to try to develop a system for managing them, eg, a list of traits or attributes one can apply to certain groups. For example, patients of Asian origin prefer _______. However, there is an inherent danger in doing this, as it leads to stereotyping [25]. Cultural factors also may be given inappropriate meaning. Specifically, a well-meaning clinician might attribute certain characteristics to a patient when in fact it has little bearing on the patient’s perspective [25]. In addition, given the nature of communication, travel, and the fact that many individuals identify with more than one cultural group, it may be inappropriate to attribute a singular cultural identity to a group in contemporary society. As a result, Kleinman [25] proposed an ethnographic approach as opposed to a cultural approach. Specifically, this involves understanding a patient and his/her illness from an individual’s perspective as opposed to the cultural collective.
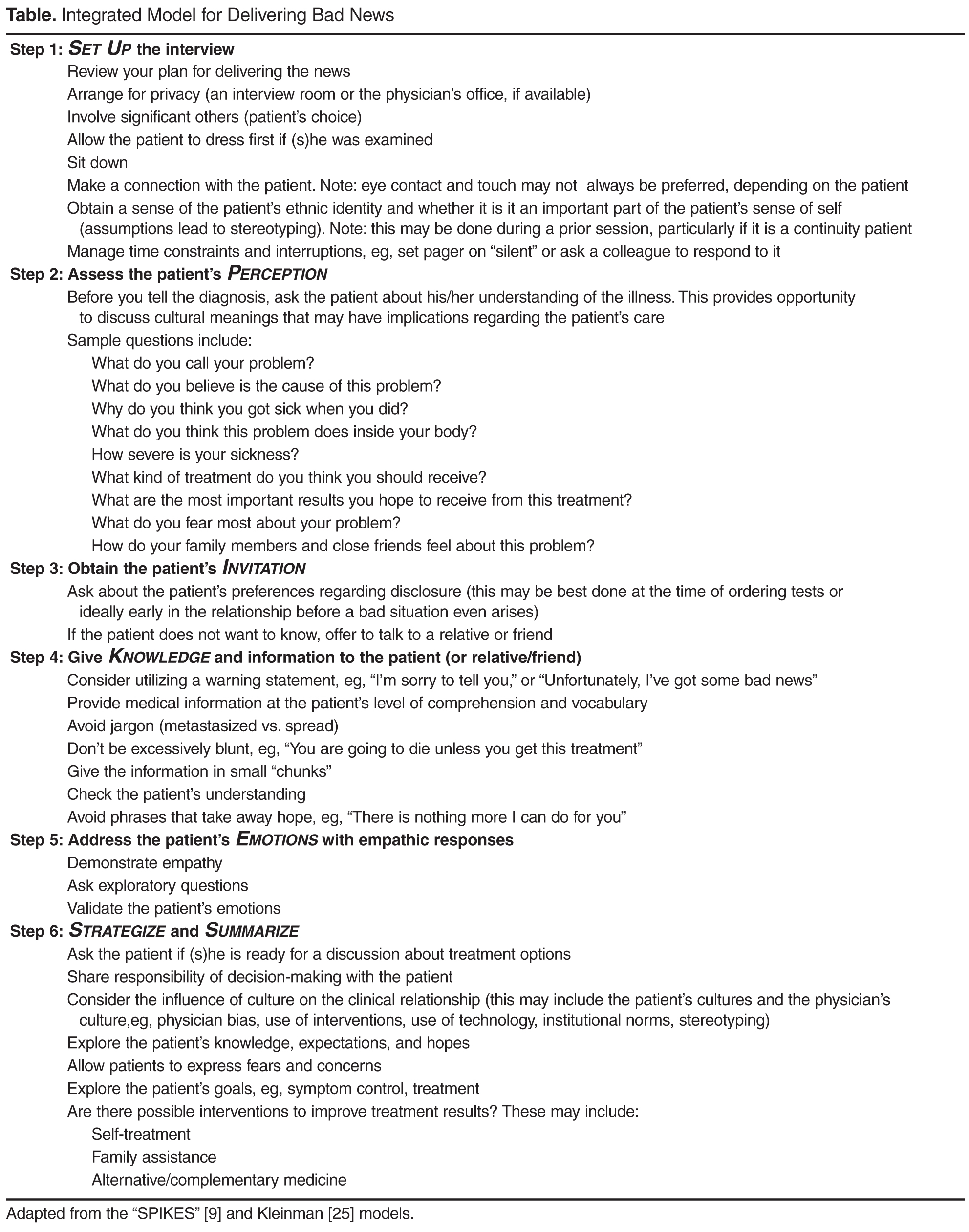
Communication Skills to Help Deliver Bad News