Coexisting Frailty, Cognitive Impairment, and Heart Failure: Implications for Clinical Care
Journal of Clinical Outcomes Management. 2015 January;22(1)
References
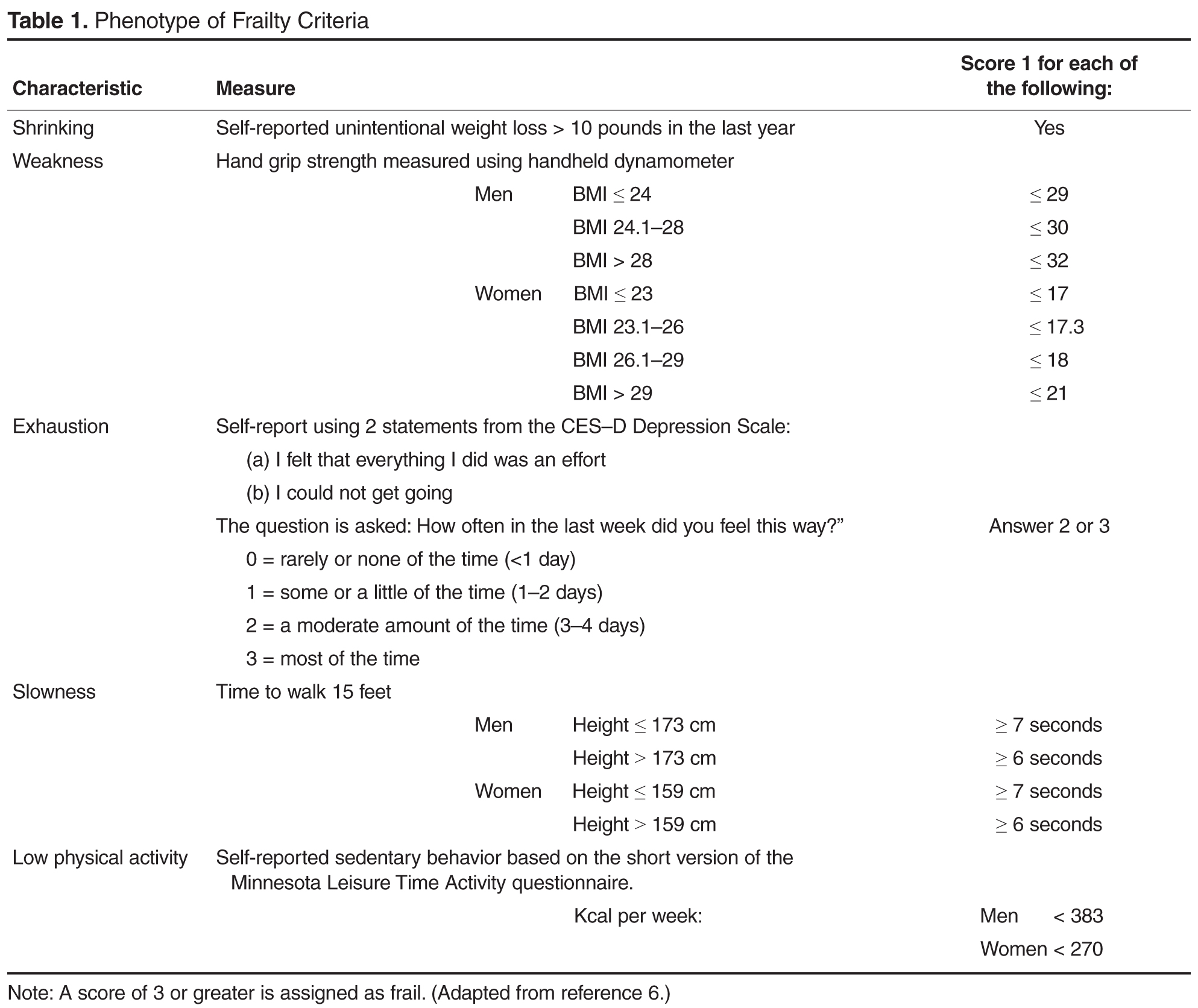
The Fried phenotype assesses 5 criteria: shrinking, weakness, exhaustion, gait speed and physical activity ( Table 1 ) [6]. A score of 0 or 1 is assigned to each of the 5 criteria and summed to get a total frailty score. Scores of 3 or greater are assigned as frail, while scores of less than 3 are considered non-frail. Scores of 1 or 2 can also be assigned as intermediate or at-risk for frailty (pre-frail). The focus of the Fried phenotype on physical domains makes it a particular appropriate measure to consider in the heart failure population since physical function declines occur as disease severity worsens.
Short Physical Performance Battery
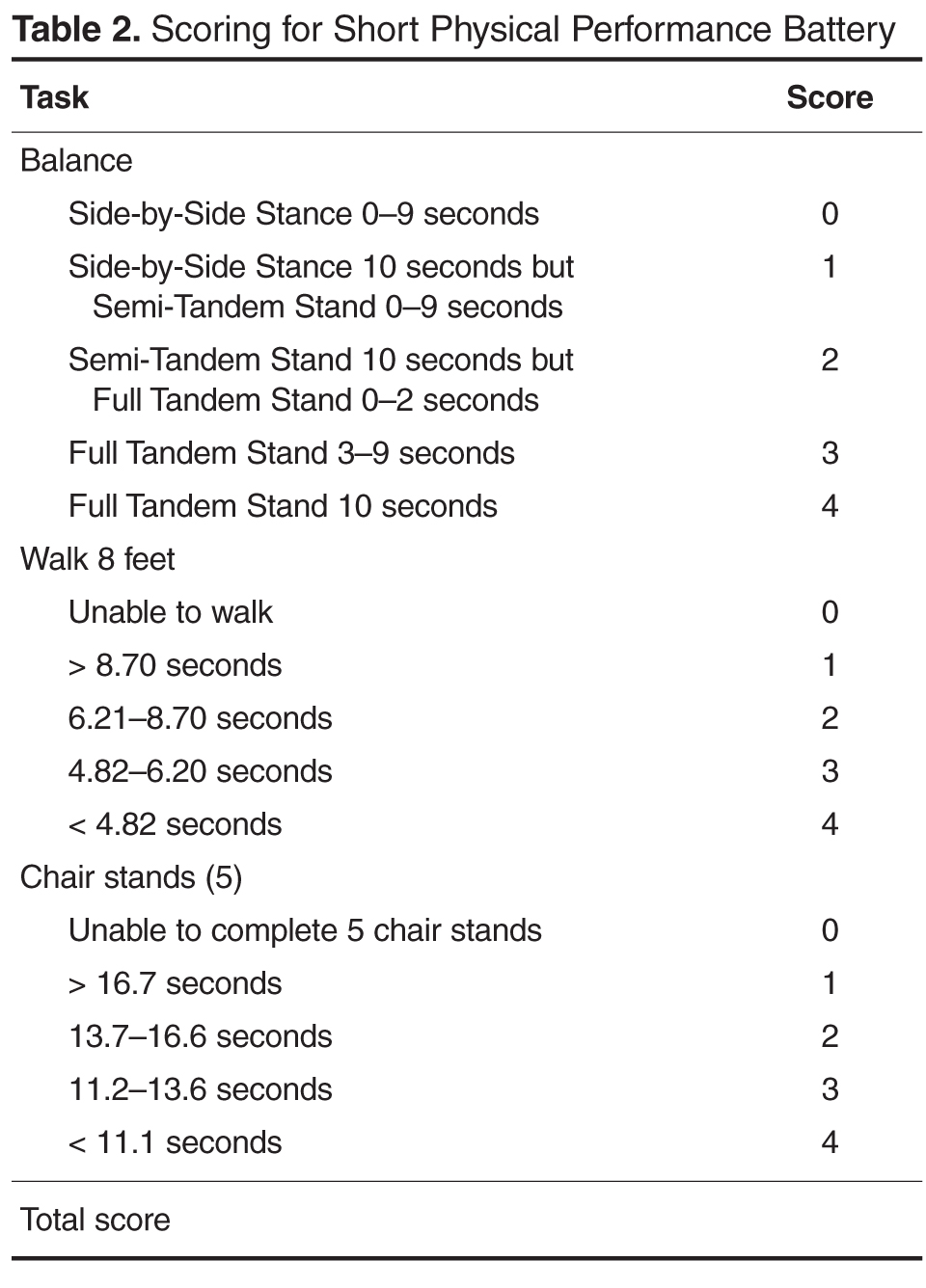
The SPPB has been used to evaluate frailty risk in older adults with heart failure [49,50]. The SPPB assesses lower extremity physical performance by testing balance, walking, and muscle strength ( Table 2 ). Scores on the SPPB are easy to interpret for clinicians, with a change of 5 clinically meaningful. Three studies have evaluated outcomes using the SPPB as a risk assessment of frailty in older adults with heart failure. Di Bari et al compared SPPB scores and the 6-minute walk test distance (6MWD) in older adults with and without heart failure [51]. SPPB scores and 6MWD were lower and predicted poor clinical outcomes in patients with heart failure compared with those without heart failure. The SPPB was used by Chiarantini et al to assess whether the SPPB predicted the long-term survival of 157 older adults (mean age, 80 yr) discharged following a heart failure exacerbation [52]. The mean SPPB score was 4.5 but varied considerably by NYHA class (class I: 7.4 ± 1.1; class II: 5.0 ± 0.5; class III: 4.8 ± 0.5; class IV: 2.3 ± 0.7; P < 0.001). Poorer SPPB scores were associated with higher mortality rates; compared with a SPPB score of 9 to 12, scores of 0, 1 to 4, and 5 to 8 were associated with mortality risks of 6.06, 4.78, and 1.95, respectively. Importantly, of approximately 30% ( n = 47) of participants who scored 0 on the SPPB, 47% were NYHA class IV and 74% were unable to perform any of the 3 tests on the SPPB. An average of 10 to 15 minutes were required to administer the SPPB in these frail, elderly hospitalized heart failure patients and no adverse events were reported.
In other chronic illness populations, the SPPB has also been used as a predictor of outcomes before, during, or after hospitalization. Valpato et al [53], for example, used the SPPB to assess older adults (mean age, 78 yr) admitted to the hospital with a diagnosis of heart failure (64%), pneumonia (13%), chronic obstructive pulmonary disease (16%), or minor stroke (6.6%) at admission (baseline) and discharge. Patients with the lowest SPPB quartile scores at hospital discharge had a fivefold greater risk of rehospitalization or mortality compared to the highest quartile. In addition, those who had an early decline in SPPB scores 1 month after hospital discharge had greater limitations in performing activities of daily living and a significantly greater probability of being re-hospitalized or death during the 1-year follow-up period. These studies suggest that the SPPB at the first follow-up outpatient visit following hospital discharge may be beneficial for identifying need for further intervention or the need for more frequent follow-up care. Although the SPPB is not part of the Fried et al phenotype, it may provide additional information concerning risk for falls and lower extremity strength that may be beneficial in the evaluation of some persons with heart failure [54]. The SPPB along with instructions and normative data are available for clinical use at no charge at www.grc.nia.nih.gov/branches/ledb/sppb/index.htm.