Management of Acute Decompensated Heart Failure in Hospitalized Patients
Journal of Clinical Outcomes Management. 2015 April;22(4)
References
How are patients with ADHF classified?
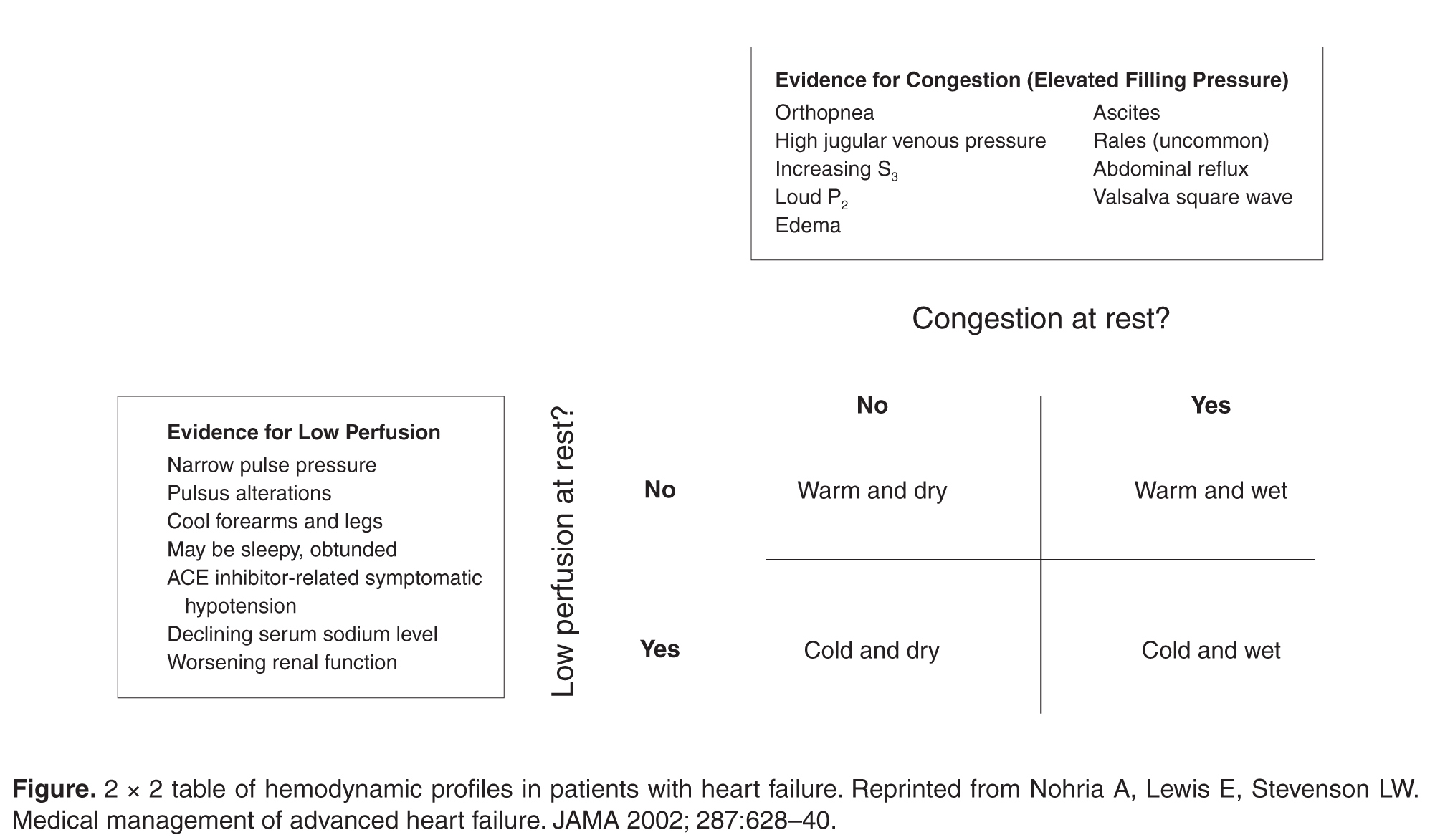
ADHF denotes the development of progressive signs and symptoms of distress that require hospitalization in patients with a previous diagnosis of heart failure. The American College of Cardiology Foundation/American Heart Association (ACCF/AHA) guideline for the diagnosis and management of heart failure in adults notes that the hospitalized patient with heart failure can be classified according to adequacy of systemic perfusion and volume status [5]. Most patients can be classified during bedside assessment according to the diagram shown in the Figure. Patients with fluid overload who present with adequate peripheral perfusion and signs and symptoms of congestion and are classified as “warm and wet.”
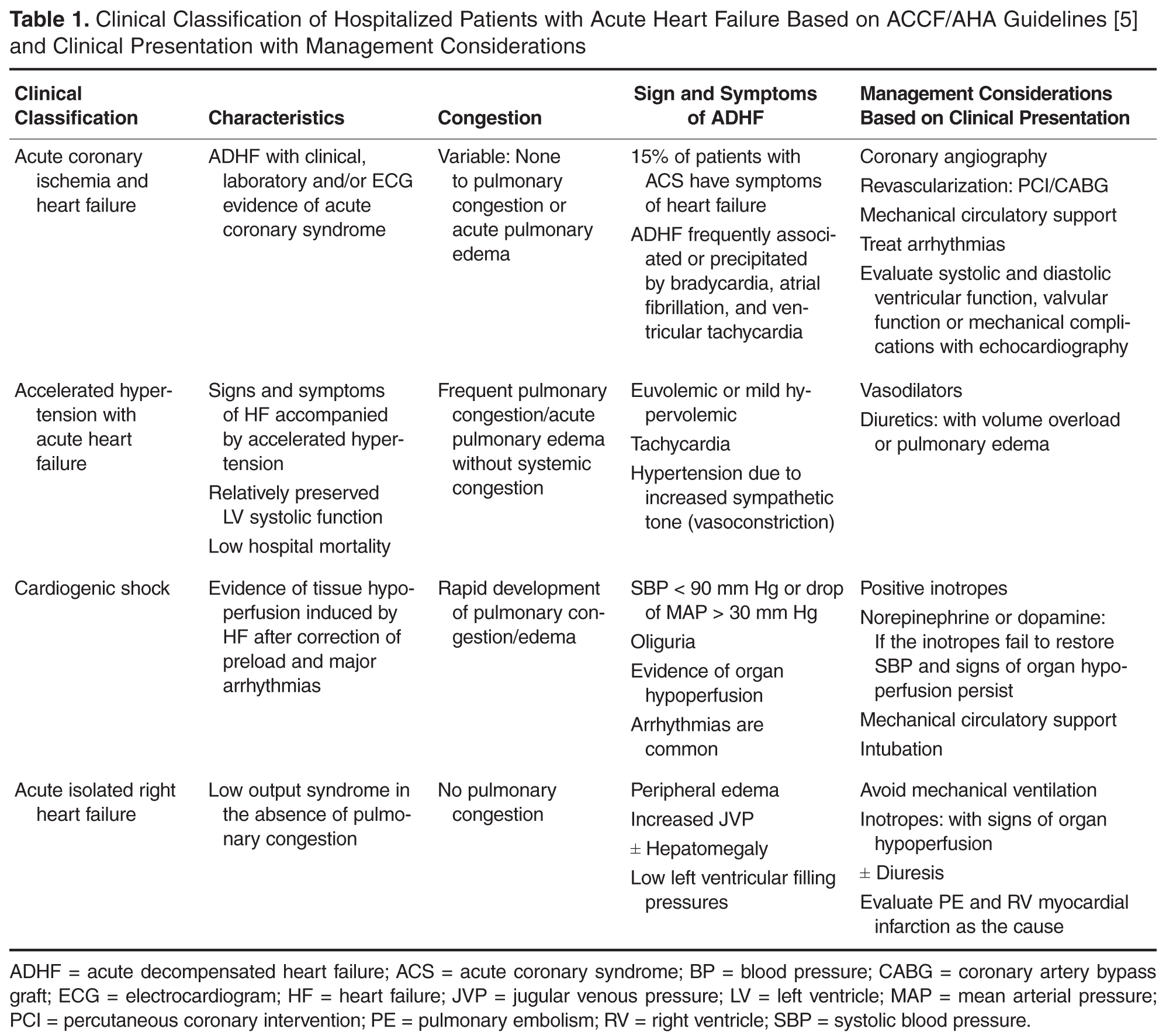
Patients without congestion but with low output with evidence of tissue hypoperfusion due to heart failure are “cold and dry,” and display a continuum of severity manifested by hypotension, renal insufficiency and/or shock. Patients with fluid overload and tissue hypoperfusion or shock are “cold and wet” [5]. Although these clinical profiles differ in their prognostic significance, clinicians should recognize the need for urgent therapy based upon clinical signs and symptoms [6]. Specifically, cold and wet patients may need observation in the cardiac care unit setting, and treatment should be directed at improving tissue perfusion and relieving congestion. The ACCF/AHA guideline also classifies hospitalized patients with ADHF into subgroups with distinct clinical and hemodynamic characteristics that require special attention. These include patients with acute coronary ischemia, accelerated arterial hypertension in patients with signs and symptoms of heart failure, shock, and acutely worsening right heart failure ( Table 1 ) [5].
What risk assessment tools are available?
B-type natriuretic peptide (BNP) and N-terminal fragment proBNP (NT-proBNP) were recently validated as diagnostic aids for the differentiation of etiologies of dypnea in patients in the ED with possible symptoms of ADHF. Use of these biomarkers can help reduce diagnostic uncertainty and associated mismanagement of patients presenting with nonspecific symptoms of dysp-nea [4,5,7]. Low or normal levels (BNP < 100 pg/ml or NT-proBNP < 500 pg/ml) have a high negative predictive value for excluding heart failure.
Elevated BNP or NT-proBNP levels may also yield prognostic information, identifying patients at increased risk of mortality or rehospitalization when value does not fall after aggressive heart failure management [8,9].In a recent study by Fonarow et al, the levels of BNP on hospital admission correlated directly with the risk of in-hospital mortality in patients admitted with ADHF independent of left ventricular ejection fraction. When the levels of BNP were below 430 pg/ml, the in-hospital mortality was 1.9%, and when the levels were above 1730 pg/ml, the mortality went up to 6% (P < 0.001) [8]. Additionally, elevated pre-discharge BNP levels (BNP > 350 ng/l; P < 0.001) in patients with ADHF seem to identify those at increased risk of death or readmission after in-patient management [9]. Elevated cardiac troponin T or I in hospitalized patients with ADHF also are associated with increased mortality, including in those without acute coronary syndrome or underlying coronary artery disease [10,11].
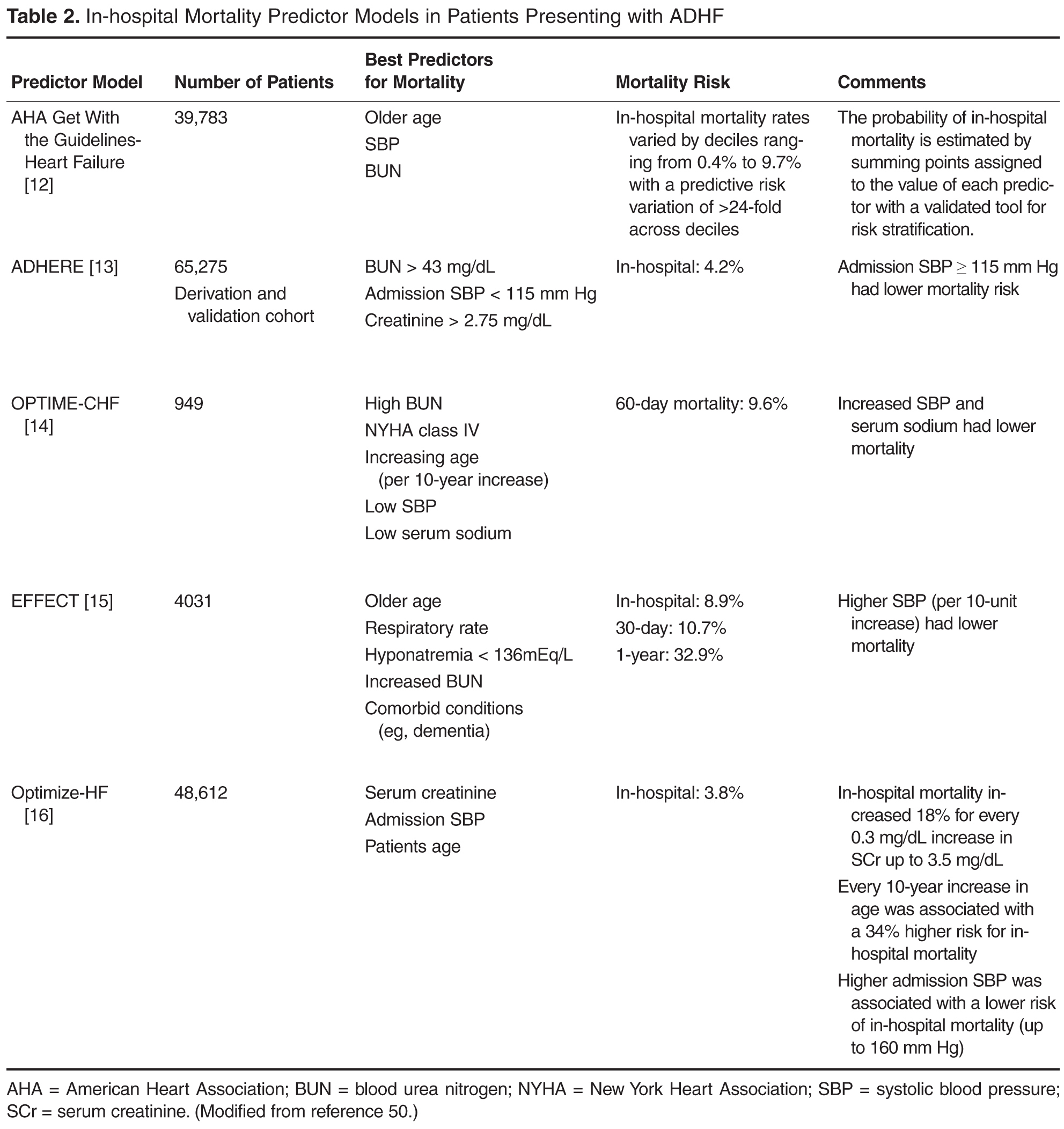
The American Heart Association Get With The Guidelines–Heart Failure (GWTG-HF) developed a validated risk score to predict in-hospital mortality in patients hospitalized for heart failure that uses commonly available clinical variables. The admission variables that were most predictive of in-hospital mortality were BUN, systolic blood pressure, and age [12]. In addition, Fonarow et al published a detailed in-hospital mortality risk stratification tool for ADHF derived from more than 65,000 patients in the ADHERE registry database [13]. Of 39 variables, high admission BUN level (≥ 43) was the best single predictor for mortality, followed by an admission systolic blood pressure less than 115 mm Hg and a serum creatinine level above 2.75 mg/dL. These variables underscore the importance of renal function as a predictor of cardiac outcomes among hospitalized patients with ADHF. Other risk stratification models and predictors of mortality in hospitalized patients with ADHF have recently been published ( Table 2