Theoretical Base
The theoretical basis for this approach is general system theory and its medical derivative, the biopsychosocial (BPS) model [11]. In describing prevalent but overlooked behavioral health problems of patients attending our CPC, we underscore the importance of the BPS model relative to the prevailing biomedical, disease-only model. The latter does not include behavioral or psychosocial dimensions, the result being that they are largely excluded from medical education and, hence, overlooked in practice. The BPS model provides the theoretical basis for including these behavioral health patients in teaching and care.
Patients
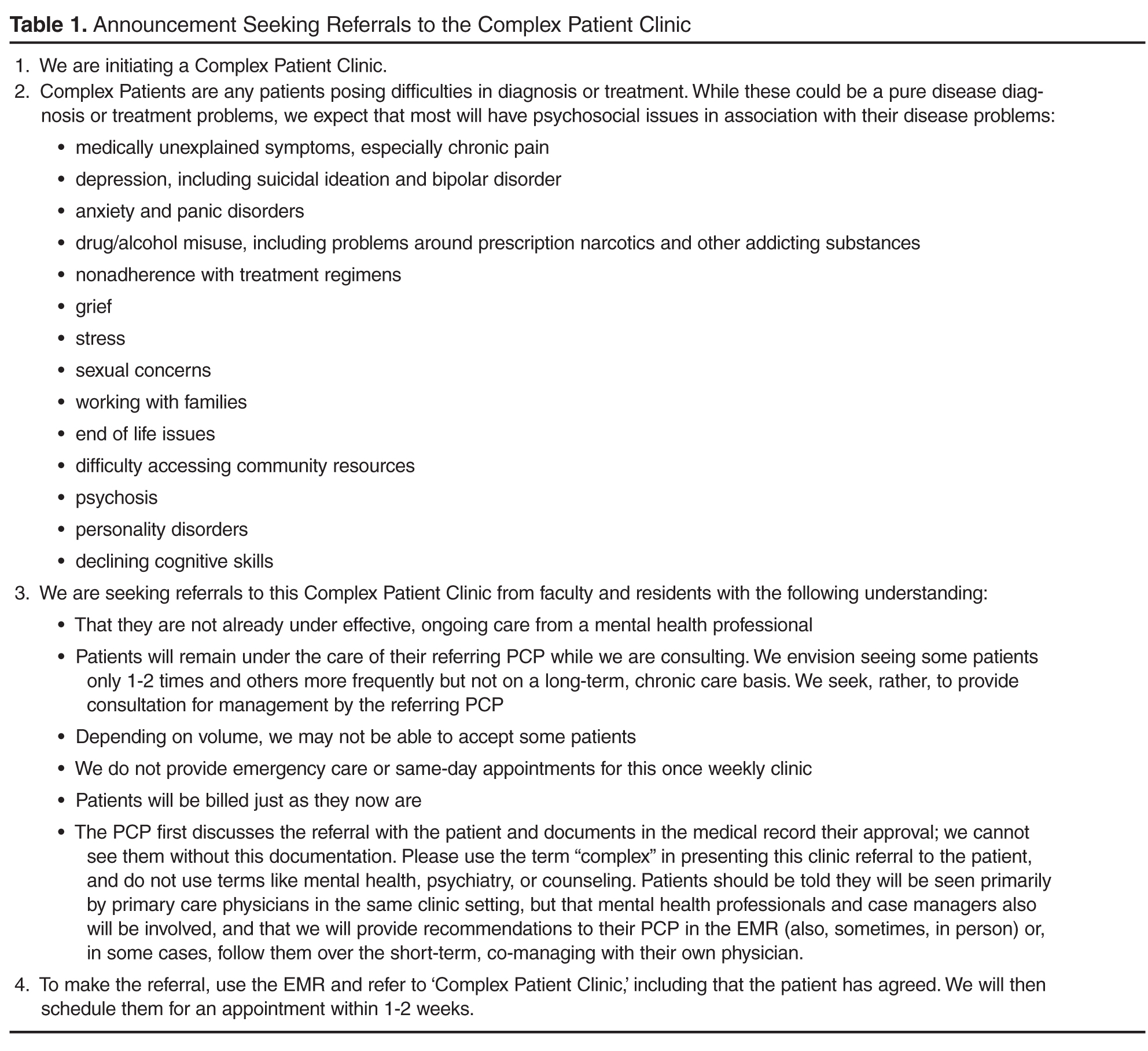
Table 1 presents the flyer sent to internal medicine and family medicine residents and faculty to request referrals to the CPC. It indicates the types of patients to consider, emphasizing any difficult diagnostic or treatment problem such as patients with medically unexplained symptoms, depression, anxiety, and substance abuse; the flyer also indicates that emergency patients and patients already under care of a psychiatrist are excluded. Patients were referred by specialist and primary care faculty as well as residents via the electronic medical record (EMR). Referring physicians discussed the referral with the patient and obtained their approval. They emphasized that the CPC was in the same clinic area, that it was supervised by both medical and psychiatry faculty, that they would be seen by medical physicians being trained, that the same clinic case manager would be involved, that video monitoring of their interaction would be requested for teaching purposes, and that they, as referring physician, would continue to be involved in care. Patients registered at the usual desk, waited in the regular clinic waiting room, and were escorted into the room by the clinic medical assistant who explained the consent procedure for monitoring and reviewed the form they would be asked to sign. The resident (or faculty) trainee requested that the interaction be observed via the computer. If signed permission was not obtained, the consultation proceeded without video monitoring. Two patients refused to sign permission. Institution review board approval was obtained for the project.
Observations
The CPC uses 3 examination rooms for one half-day a week in the usual resident and faculty area of the Clinical Center of Michigan State University Department of Medicine. Rooms are similar to other clinic examination rooms except that a second computer attached to small audio video recorder is placed on the physician’s desk. Visible to the patient, it broadcasts live the patient-resident interaction to a nearby room where teaching faculty observe the interaction on a computer linked by a special software program (Vidyo, Hackensack, NJ) [12]. Access and control of Vidyo virtual rooms is restricted and rooms can only be entered by participating faculty using pre-assigned usernames and passwords. No recordings of the interactions are made.
Training faculty and the resident reviewed the patient’s EMR before each interaction and faculty continued to review it while observing the interaction. Both faculty and trainee documented information in the EMR in the fashion used with other patients.
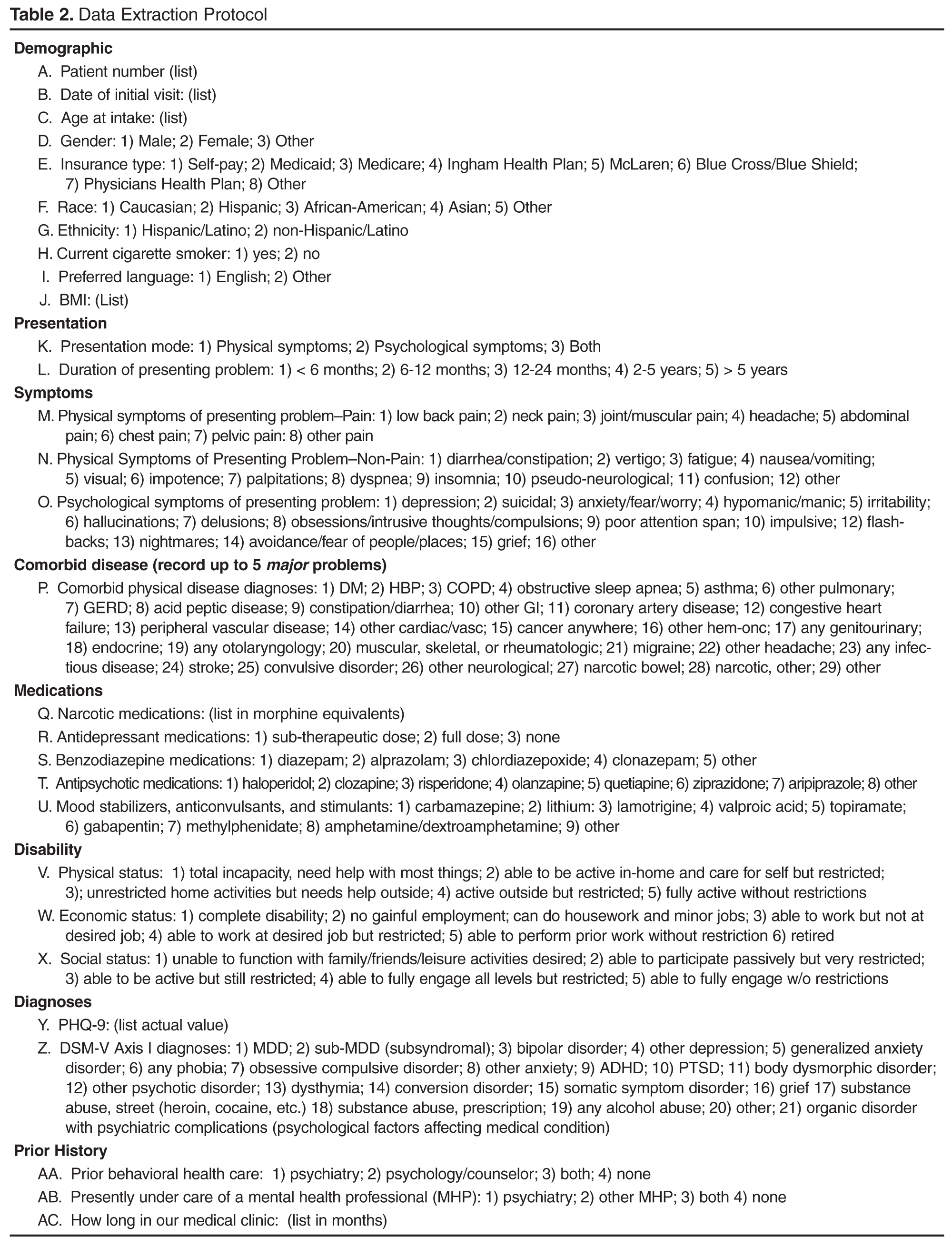
Data