Telepsychiatry is an approach, where by EDs that do not have access to psychiatrists can see patients in the ED itself, by forming a contract with either psychiatrists or companies to allow a psychiatrist at another location to perform an examination on a patient via video connection and advise the emergency room providers on treatment and intervention. There is very little data in the peer-reviewed literature on the use of telepsychiatry. The literature is limited to case reports, program descriptions, and randomized studies for reliability.67,68 One randomized controlled trial showed that a telepsychiatry evaluation had a reliable diagnosis and disposition when compared to a face-to-face assessment.69 One case control showed reduction in time-to-consult done in the ED, length of stay, and door-to-consult stay, once a telepsychiatry program was initiated.70 A large case control study showed that telepsychiatry recipients were more likely to receive 30-day follow-up, 90-day follow-up, and total inpatient length of stay, totaling both initial admission and subsequent admissions.71 Therefore, it is reasonable for EDs to take advantage of telepsychiatry services if no immediate psychiatrist coverage is available.
Disposition
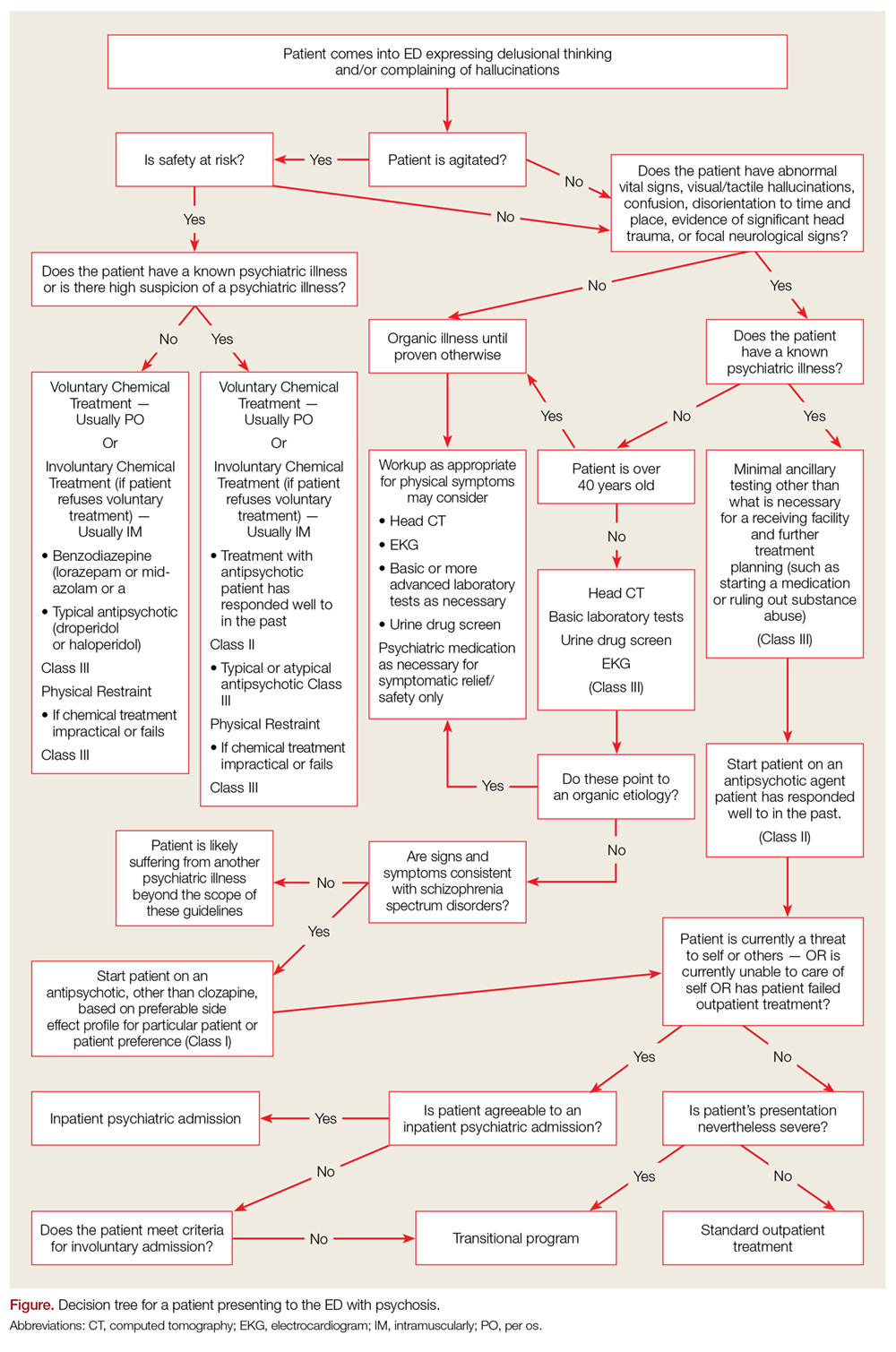
The primary disposition question regarding a patient presenting with a psychiatric chief complaint to the ED, including schizophrenia, is whether they require a psychiatric admission or not. If a patient requires hospitalization but refuses, the emergency clinician must decide if the patient meets criteria for involuntarily hospitalization. If a patient does not require an inpatient admission or would benefit from an inpatient admission but does not meet criteria for civil commitment, then the next major question is what type of outpatient treatment is sufficient for this particular patient (Figure).
Figure.
For a patient with schizophrenia to require inpatient psychiatric admission he must be either a danger to himself or others or has failed outpatient treatment. In addition, the patient must currently have undergone a clinical evaluation of any suspected medical illness, and any medical problems the patient is experiencing must be sufficiently stable to allow safe transport and treatment at a psychiatric hospital unit.9 If a patient’s medical condition is not sufficiently stable for either transport or hospitalization at a psychiatric hospital but the patient still requires inpatient psychiatric treatment, the patient should be hospitalized on a standard medical ward and receive psychiatric care on that unit.
Patients with mental illness pose an additional challenge, in that their illness often time interferes with their judgment about whether they require treatment. Because of this possible lack of capacity and the potential danger of a patient with mental illness to self or others, most jurisdictions have a legal code that allows for involuntary hospitalization of the mentally ill. However, which patients qualify for involuntary hospitalizations vary by jurisdiction. Case law criteria for emergencies range from a risk of “imminent” harm to self or others to a deterioration in the patient’s mental condition if treatment is halted.72 Providers are recommended to familiarize themselves with laws regarding inpatient civil commitment in their particular jurisdiction.
When a patient is being discharged from the ED, either because they do not require a psychiatric inpatient admission or because they don’t meet criteria for involuntary commitment, there are various outpatient dispositions available. Any patient with a diagnosis of schizophrenia should have outpatient follow-up with a mental health provider upon discharge from the ED.
For patients who have a failed community treatment in the past, who do not have a significant support network, or whose disease is too severe for a regular outpatient clinic to handle would be better suited for a disposition to a transitional program over a standard outpatient appointment; such as partial hospitalization programs, intensive outpatient programs, and community mental health treatment teams (CMHT). Assertive community treatment (ACT) teams are a form of CMHT comprised of several disciplines, including nurses, occupational therapists, psychiatrists, psychologists, and social workers.73 A large prospective cohort study found homeless patients to have made gains in multiple spheres of mental health while enrolled in ACT programs, and these benefits were retained after discharge from the ACT program.74
Conclusion
Schizophrenia is characterized primarily by delusions, hallucinations, and disorganized thinking. Emergency medicine providers are frequently at the front lines of diagnosing, initiating treatment, and managing relapses for these individuals. As schizophrenia is an exclusion, the primary task of an emergency physician is to rule out all “organic”, for lack of a better term, causes of the psychosis or disordered thinking before making a definitive diagnosis of schizophrenia. As many EDs do not have sufficient psychiatry support and many patients with schizophrenia are using the ED as their location for primary mental health, many emergency physicians are finding themselves acting as the main providers for these individuals. The primary treatment for patients with schizophrenia remains monotherapy with antipsychotic medication. Although the highest-level disposition for a patient with schizophrenia remains the inpatient psychiatry department, there are many transitional dispositions that can bridge the gap between a discharge to standard community care and an inpatient admission.