SGLT2 Inhibitors for Type 2 Diabetes Mellitus Treatment
SGLT2 inhibitors are plausible second-line drugs that provide powerful additional A1c-lowering effects while inducing weight loss without hypoglycemia.
Dr. Plodkowski is a former chief of endocrinology and Dr. Nguyen was an endocrinologist at the VA Sierra Nevada Health Care System in Reno. Dr. Plodkowski, Dr. McGarvey, and Dr. Huribal are endocrinologists in the Division of Endocrinology, and Dr. McGarvey is also the associate program director of the Endocrinology Fellowship, all at Scripps Clinic in San Diego. Dr. Nguyen is the medical director of Las Vegas Endocrinology and an adjunct associate professor of medicine at Touro University Nevada College of Osteopathic Medicine, both in Nevada, and a clinical associate professor of clinical education at Arizona College of Osteopathic Medicine in Glendale, California. Mr. Reisinger-Kindle and Mr. Kramer are medical students at Touro University Nevada College of Osteopathic Medicine. Dr. Solomon is a senior medical resident at Valley Hospital Medical Center/Touro University.
References
Over the past 2 decades, the treatment of type 2 diabetes mellitus (T2DM) has been an evolving science. With therapeutic advances, the prevalence of catastrophic complications such as amputations, renal failure requiring dialysis, and blindness due to retinopathy have significantly declined. Developed drugs have successfully met treatment goals; however, they are often associated with a higher risk of hypoglycemia and weight gain. Now that better glucose control is possible, the science of diabetes care continues to evolve. Newly developed drugs should control glucose without significant hypoglycemia and also promote weight reduction. The sodium-glucose transport protein 2 (SGLT2) inhibitor drug class has these characteristics, and the novel mechanism of action complements older medications used to treat T2DM.
Phlorizin is a plant-based compound originally discovered in 1935 when it was derived from the bark of apple trees. 1 It is a naturally occurring botanical glucoside and is fairly nonselective between SGLT1 and SGLT2. Due to its poor bioavailability and its degradation in the gastrointestinal tract, it was not an ideal drug candidate in humans.
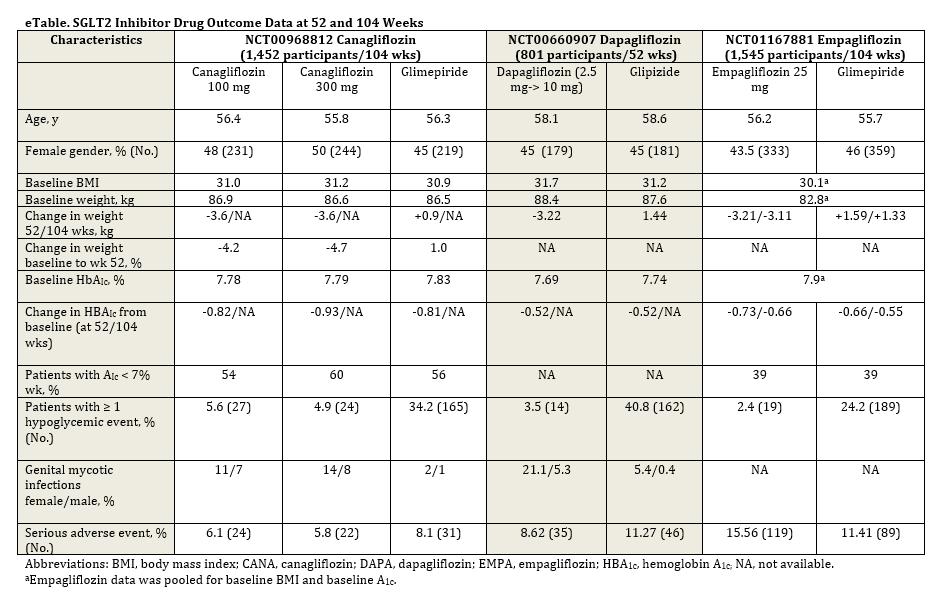
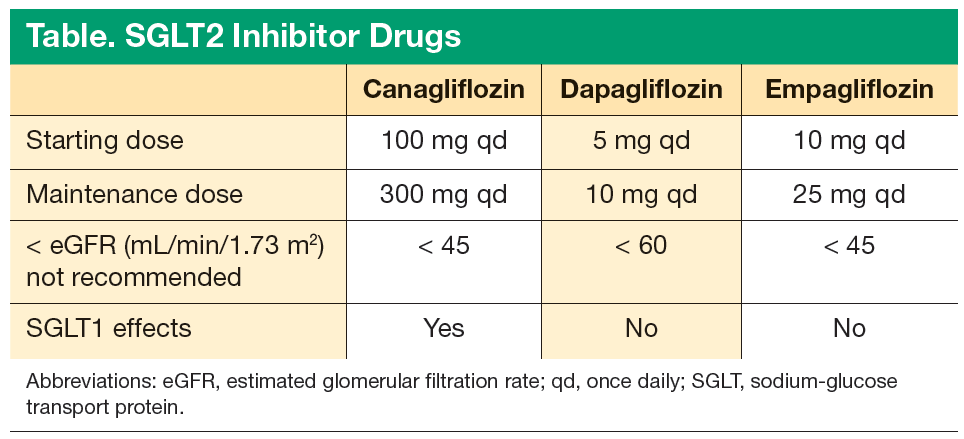
However, it stood as a starting point for the development of the current gliflozin class of SGLT2 inhibitors canagliflozin, dapagliflozin, and empagliflozin, which are reviewed in this article. The Table outlines the differences between the drugs. The eTable highlights clinical trial data for each drug.
Canagliflozin
Canagliflozin is a SGLT2 inhibitor and a low-potency SGLT1 inhibitor. It was the first SGLT2 inhibitor approved by the FDA (March 2013) to be used with diet and exercise to improve glycemic control in adults with T2DM. The recommended starting dose is 100 mg once daily for patients who have an estimated glomerular filtration rate (eGFR) > 60 mL/min/1.73m2 and can be increased to 300 mg once daily. It is also available in a fixed-dose combination with metformin. Canagliflozin SGLT-2 inhibition leads to increased glycosuria and osmotic diuresis that lowers plasma glucose concentrations. Lower blood pressure (BP) is likely an effect of the osmotic diuresis. Increased urinary excretion of glucose also leads to a loss of calories and weight loss. It was studied alone and in combination with metformin, sulfonylurea, pioglitazone, and insulin therapy.
The pharmacokinetics of canagliflozin is similar in healthy subjects and patients with T2DM. Peak plasma concentrations (C max) and area under the cover (AUC) of canagliflozin increased in a dose-proportional manner from 50 mg to 300 mg. Following single-dose oral administration of 100 mg and 300 mg of canagliflozin, time to C max (T max) of canagliflozin occurs within 1 to 2 hours postdose. The apparent terminal half-life (t1/2) was 10.6 hours and 13.1 hours for the 100 mg and 300 mg doses, respectively. Steady state was reached after 4 to 5 days of once-daily dosing with canagliflozin 100 mg to 300 mg. Glucuronidation is the major metabolic pathway. There is balanced renal and biliary excretion of metabolites, and there are no active metabolites.
Following oral doses of canagliflozin in patients with T2DM, dose-dependent decreases were seen in the renal threshold for glucose (RTG). From a starting value of about 240 mg/dL, the 300-mg dose suppressed the mean (RTG) to about 70 to 90 mg/dL in T2DM in phase 1 studies. The reduction in RTG led to increase in urinary excretion of glucose of about 100 g/d.