By Kensuke Adachi, MD, PhD, and Kazuaki Enatsu, MD.
Published previously in Gastroenterology (2013;144[1]:32, 251).
A previously healthy, 56-year-old man visited our hospital with a 2-month history of dysphagia. The patient’s past medical history was unremarkable. He denied a recent history of weight loss, reflux symptoms, or food impaction. Laboratory and physical test results revealed no abnormalities. Barium swallow esophagogram showed dilatation of the esophagus with a filling defect, approximately 7 cm long, in the intrathoracic esophagus (Figure A).
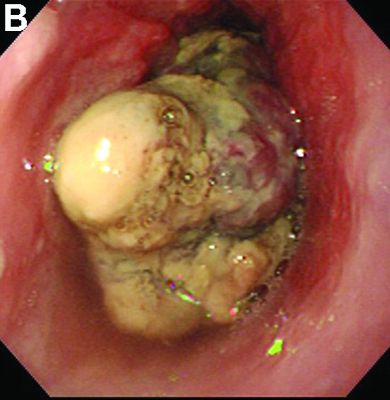
Endoscopy also revealed an elastic and large polypoid tumor occupying the almost whole lumen in the mid-esophagus (Figure B). Despite such a bulky appearance, the lesion allowed easy passage of the endoscope into the stomach. Endoscopic biopsy specimens suggested a malignant tumor of the esophagus. There were no suspicious lymph nodes or distant metastases on preoperative computed tomography. The patient underwent an esophagectomy and standard three-field lymphadenectomy with gastric replacement via the posterior mediastinal route and intrathoracic anastomosis. He had an uneventful recovery and was discharged on postoperative day 11. The operative specimen is shown in Figure C.
According to the TMN classification, the postoperative diagnosis was T2N0M0, equivalent to stage IIA. Fortunately, the patient was alive and free of recurrence after 7 years of follow-up.