Marc Rosen is the Director of Addictions Firm, Steve Martino is the Chief of Psychology, John Sellinger is the Director of Clinical Health Psychology, Brenda Fenton is the Associate Director, Methods and Biostatistics Core, PRIME Center; all at VA Connecticut Healthcare System in West Haven. Kristin Mattocks is the Associate Chief of Staff for Research at the VA Central Western Massachusetts Healthcare System in Leeds. Marc Rosen and Steve Martino are Professors of Psychiatry, John Sellinger is an Assistant Professor of Psychiatry, and Christina Lazar is a Research Associate, all at Yale University in New Haven, Connecticut. Kristin Mattocks is an Associate Professor of Population and Quantitative Health Sciences at the University of Massachusetts Medical School in Worcester. Correspondence: Marc Rosen (marc.rosen@yale.edu)
Author disclosures The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the US Government, or any of its agencies.
Background: The Compensation and Pension (C&P) determination process is a potential gateway to accessing pain treatment in the Veterans Health Administration (VHA). However, attitudes about C&P as a gateway and about collaboration with C&P clinics among VHA staff are unknown.
Methods: In preparation for an initiative to link veterans seeking compensation for musculoskeletal disorders to treatment, clinical and administrative staff from the 8 VHA medical centers in New England were invited to complete a relational coordination survey that examined how different workgroups collaborate (communication and relationships) to provide pain care to veterans. A subset of those staff also participated in a semistructured interview about pain treatment referral practices within their medical centers. VHA staff were from primary care, administration, pain management, and C&P teams.
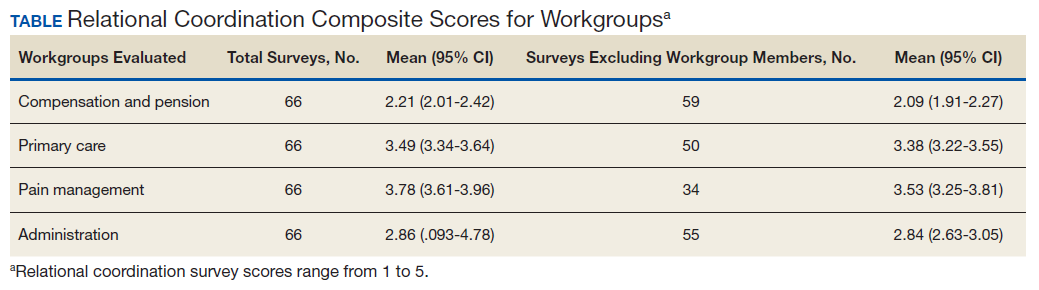
Results: Eighty-three VHA staff were invited to complete the relational coordination survey; 66 completed the survey and 39 participated in the semistructured interview. Most C&P staff interviewed thought of the compensation examination as a forensic process and that C&P-based efforts to engage veterans might interfere with the examination or were not their responsibility. However, some examiners described their efforts to determine new veterans’ eligibility for VHA care and to connect them to specific treatments. VHA staff reported that there was little communication between the C&P team and other teams. The survey results supported this finding. The C&P group’s relational coordination composite scores were lower than any other workgroup.
Conclusion: Outreach to veterans at New England C&P clinics was inconsistent, and C&P teams rated low on a measure of coordination with workgroups involved in pain treatment. Compensation examinations appear to be underused opportunities to help veterans access treatment. C&P-based treatment engagement is feasible; it is being done by some Compensation teams.
Chronic pain is common in veterans, and early engagement in pain treatment is recommended to forestall consequences of untreated pain, including depression, disability, and substance use disorders. The Veterans Health Administration (VHA) employs a stepped care model of pain treatment, with the majority of pain care based in primary care (step 1), and an array of specialty/multimodal treatment options made available at each step in the model for patients with more complex problems, or those who do not respond to more conservative interventions.1
Recognizing the need for comprehensive pain care, the US Congress passed the Comprehensive Addiction and Recovery Act, 21 USC §1521 (2016), which included provisions for VHA facilities to offer multimodal pain treatment and to report the availability of pain care options at each step in the stepped care model.2, With the passage of the Veterans Access, Choice, and Accountability Act of 2014, 38 USC §101 (2014) and now the MISSION Act of 2018, 38 USC §703 (2018) veterans whose VHA facilities are too distant, who require care unavailable at that facility, or who have to wait too long to receive care are eligible for treatment at either VHA or non-VHA facilities.3 These laws allocate the same pool of funds to both VHA and community care and thus create an incentive to engage veterans in care within the VHA network so the funds are not spent out of network.4
An opportunity to connect veterans with VHA care arises at specialized VHA Compensation and Pension (C&P) clinics during examinations that determine whether a veteran’s health conditions were caused or exacerbated by their military service. Veterans file claims with the US Department of Veterans Affairs (VA) Veterans Benefits Administration (VBA), which sends the patient to either a VHA facility or private practitioners for these examinations. Although the number of examinations conducted each year is not available, there were 274,528 veterans newly awarded compensation in fiscal year 2018, and a substantial number of the total of 4,743,108 veterans with C&P awards had reevaluation examinations for at least 1 of their conditions during that year.5 Based largely on the compensation examination results, military service records, and medical records, veterans are granted a service-connected rating for conditions deemed related to military service. A service-connection rating between 0% and 100% is assigned by the VBA, with higher ratings indicating more impairment and, consequently, more financial compensation. Service-connection ratings also are used to decide which veterans are in the highest priority groups for receipt of VHA health care services and are exempt from copayments.
Although traditionally thought of as a forensic evaluation with no clinical purpose, the C&P examination process affords many opportunities to explain VHA care to veterans in distress who file claims.6 A randomized clinical trials (RCT) involving veterans with mental health claims and a second RCT including veterans with musculoskeletal claims each found that veterans use more VHA services if offered outreach at the time of the C&P examination.7,8 In addition to clinical benefits, outreach around the time of C&P examinations also might mitigate the well documented adversarial aspects of the service-connection claims process.6,9,10 Currently, such outreach is not part of routine VHA procedures. Ironically, it is the VBA and not VHA that contacts veterans who are awarded service-connection with information about their eligibility for VHA care based on their award.
Connecting veterans to pain treatment can involve clarifying eligibility for VHA care for veterans in whom eligibility is unknown, involving primary care providers (PCPs) who are the fulcrum of VHA pain care referrals, and motivating veterans to seek specific pain treatment modalities. Connecting veterans to treatment at the time of their compensation examinations also likely involves bidirectional cooperation between the specialized C&P clinics where veterans are examined and the clinics that provide treatment.
Relational coordination is a theoretical framework that can describe the horizontal relationships between different teams within the same medical facility. Relational coordination theorizes that communication between workgroups is related synergistically to the quality of relationships between workgroups. Relational coordination is better between workgroups that share goals and often have high levels of relational coordination, which is thought to be especially important when activities are ambiguous, require cooperation, and are conducted under time pressure.11 High relational coordination also has been associated with high staff job satisfaction, high satisfaction with delivered services, and adherence to treatment guidelines.12-14 An observational cohort study suggested that relational coordination can be improved by targeted interventions that bring workgroups together and facilitate intercommunication.15
To better understand referral and engagement for pain treatment at compensation examinations, VA staff from primary care, mental health, pain management, and C&P teams at the 8 VHA medical centers in New England were invited to complete a validated relational coordination survey.11,16 A subset of invited staff participated in a semistructured interview about pain treatment referral practices within their medical centers.