Authors’ Disclosure Statement: Dr. Barsoum reports that he receives royalties from Stryker, Exactech, and Zimmer Biomet; a patent from Zimmer Biomet; consultant fees from Stryker; stock/stock options from iVHR, Peer Well, Custom Orthopaedic Solutions, and Otismed; research support from Stryker, Zimmer Biomet, DJO, and Orthosensor; and other financial support from KEF Healthcare. Dr. Higuera reports that he receives personal fees from Zimmer Biomet, Covance, and Pfizer; research support/grants and personal fees from KCI; and research support/grants from Stryker, Myoscience, CD Diagnostics, The Orthopaedic Research and Education Foundation (OREF), and Pacira. He is on the editorial review board of The American Journal of Orthopedics. The other authors report no actual or potential conflict of interest in relation to this article.
Periprosthetic joint infection (PJI) is a serious and potentially devastating complication of total joint arthroplasty. Accurate diagnosis of PJI is of utmost importance, but differentiating septic from aseptic failed total joint arthroplasty is extremely challenging, and improper management can lead to significant morbidity. The gold standard for PJI diagnosis is based on standardized laboratory and clinical criteria but relies on preoperative and intraoperative findings, which can be unreliable. Given these limitations, research has focused on new methods for diagnosing PJI. Synovial fluid inflammatory cytokines have been found to accurately diagnose PJI. In this article, we review the synovial fluid cytokines that are being used as aids in PJI diagnosis.
In cases of failed TJA, it is important to differentiate between septic and aseptic etiologies.
Chronic and low-grade infections are challenging for orthopedic surgeons, as the symptoms often overlap with aseptic etiologies.
Verification of infection eradication before beginning the second-stage reimplantation surgery is extremely important, but pre- and intraoperative findings can be unreliable.
Synovial fluid cytokines have been shown to accurately diagnose PJIs.
Synovial fluid cytokines may help surgeons differentiate between septic and aseptic cases of failed TJA.
Total joint arthroplasty (TJA) is an effective procedure that has been extensively used to relieve pain and improve quality of life in patients with various forms of joint disease. Although advances in technology and surgical technique have improved the success of TJA, periprosthetic joint infection (PJI) remains a serious complication. In the United States, it is estimated that PJI is the most common reason for total knee arthroplasty failure and the third most common reason for total hip arthroplasty revision.1 Although the incidence of PJI is 1% to 2%, the dramatic increase in TJA volume is expected to be accompanied by a similar rise in the number of infected TJAs; that number is expected to exceed 60,000 in the United States by 2020.2 Moreover, management of PJI is expensive and imposes a heavy burden on the healthcare system, with costs expected to hit $20 billion by 2020 in the US.2 Therefore, treating asepsis cases as infections imposes a heavy burden on the healthcare system and may result in excessive morbidity.3 At the same time, inadequate management of a PJI may result in recurrences that require infection treatment with morbid procedures, such as arthrodesis or amputation. Accurate diagnosis of PJI is of paramount importance in preventing potential implications of a misdiagnosed case. Unfortunately, the PJI diagnosis is extremely challenging, and the available diagnostic tests are often unreliable.4 Thus, research has recently focused on use of several synovial fluid cytokines in the detection of PJI.5-7 In this article, we provide an overview of the synovial biomarkers being used to diagnose PJI.
Diagnosis of Periprosthetic Joint Infection
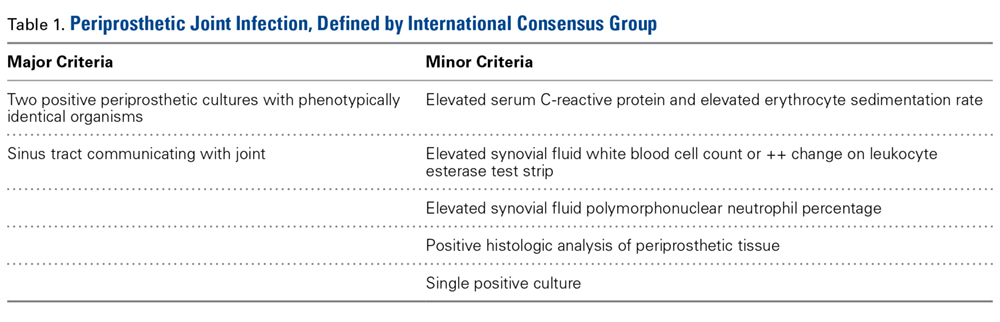
Differentiating between septic and aseptic failed TJA is important, as the treatment options differ considerably. PJI can be broadly classified as acute or early postoperative (<6 weeks), late chronic (indolent onset), and acute-on-chronic (acute onset in well-functioning prosthesis, secondary to hematogenous spread).8 The acute and acute-on-chronic presentations are often associated with obvious signs of infection.9 However, chronic and low-grade infections pose a challenge to modern orthopedic practice, as the symptoms often overlap with that of aseptic causes of TJA failure.10 As a result, the International Consensus Group on Periprosthetic Joint Infection developed complex criteria using the Musculoskeletal Infection Society definition of PJI and involving a battery of tests for PJI diagnosis.11 According to these criteria, PJI is diagnosed when 1 of the 2 major criteria or 3 of the 5 minor criteria are met (Table 1).
Table 1.
Although these criteria constitute the most agreed on and widely used standard for PJI diagnosis, the definition is complex and often incomplete until surgical intervention. An ideal diagnostic test would aid in managing a PJI and provide results before a treatment decision is made. Many revision surgeries are being performed with insufficient information about the true diagnosis, and the diagnosis might change during or after surgery. About 10% of the revisions presumed to be aseptic may unexpectedly grow cultures during surgery and thereby satisfy the criteria for PJI after surgery.12 Moreover, with the use of novel methods such as polymerase chain reaction, microorganisms were identified in more than three-fourths of the presumed aseptic revisions.13 The optimal management of such cases is controversial, and it is unclear whether positive cultures should be treated as possible contaminants or true infection.12,14