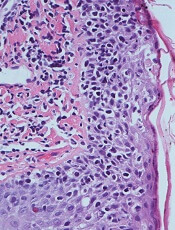
 mycosis fungoides
mycosis fungoides
Micrograph showing
The US Food and Drug Administration (FDA) has approved mogamulizumab-kpkc (Poteligeo®) for the treatment of adults with relapsed or refractory mycosis fungoides (MF) or Sézary syndrome (SS) after at least 1 prior systemic therapy.
Mogamulizumab is a humanized monoclonal antibody directed against CC chemokine receptor 4 (CCR4). It is the first biologic agent targeting CCR4 to be approved for patients in the US.
Mogamulizumab is expected to be commercially available in the fourth quarter of 2018.
The FDA previously granted mogamulizumab breakthrough therapy and orphan drug designations as well as priority review.
The FDA’s approval of mogamulizumab is supported by the phase 3 MAVORIC trial. Results from this trial were presented at the 10th Annual T-cell Lymphoma Forum in February.
MAVORIC enrolled 372 adults with histologically confirmed MF or SS who had failed at least 1 systemic therapy. They were randomized to receive mogamulizumab at 1.0 mg/kg (weekly for the first 4-week cycle and then every 2 weeks) or vorinostat at 400 mg daily.
Patients were treated until disease progression or unacceptable toxicity. Those receiving vorinostat could cross over to mogamulizumab if they progressed or experienced intolerable toxicity.
Baseline characteristics were similar between the treatment arms.
The study’s primary endpoint was progression-free survival. The median progression-free survival was 7.7 months with mogamulizumab and 3.1 months with vorinostat (hazard ratio=0.53, P<0.0001).
The global overall response rate (ORR) was 28% (52/189) in the mogamulizumab arm and 5% (9/186) in the vorinostat arm (P<0.0001).
For patients with MF, the ORR was 21% with mogamulizumab and 7% with vorinostat. For SS patients, the ORR was 37% and 2%, respectively.
After crossover, the ORR in the mogamulizumab arm was 30% (41/136).
The median duration of response (DOR) was 14 months in the mogamulizumab arm and 9 months in the vorinostat arm.
For MF patients, the median DOR was 13 months with mogamulizumab and 9 months with vorinostat. For SS patients, the median DOR was 17 months and 7 months, respectively.
The most common treatment-emergent adverse events (AEs), occurring in at least 20% of patients in either arm (mogamulizumab and vorinostat, respectively), were:
- Infusion-related reactions (33.2% vs 0.5%)
- Drug eruptions (23.9% vs 0.5%)
- Diarrhea (23.4% vs 61.8%)
- Nausea (15.2% vs 42.5%)
- Thrombocytopenia (11.4% vs 30.6%)
- Dysgeusia (3.3% vs 28.0%)
- Increased blood creatinine (3.3% vs 28.0%)
- Decreased appetite (7.6% vs 24.7%).
There were no grade 4 AEs in the mogamulizumab arm. Grade 3 AEs in mogamulizumab recipients included drug eruptions (n=8), infusion-related reactions (n=3), fatigue (n=3), decreased appetite (n=2), nausea (n=1), pyrexia (n=1), and diarrhea (n=1).