Journal of Clinical Outcomes Management. 2015 September;22(9)
References
Mechanisms of Psychological Distress
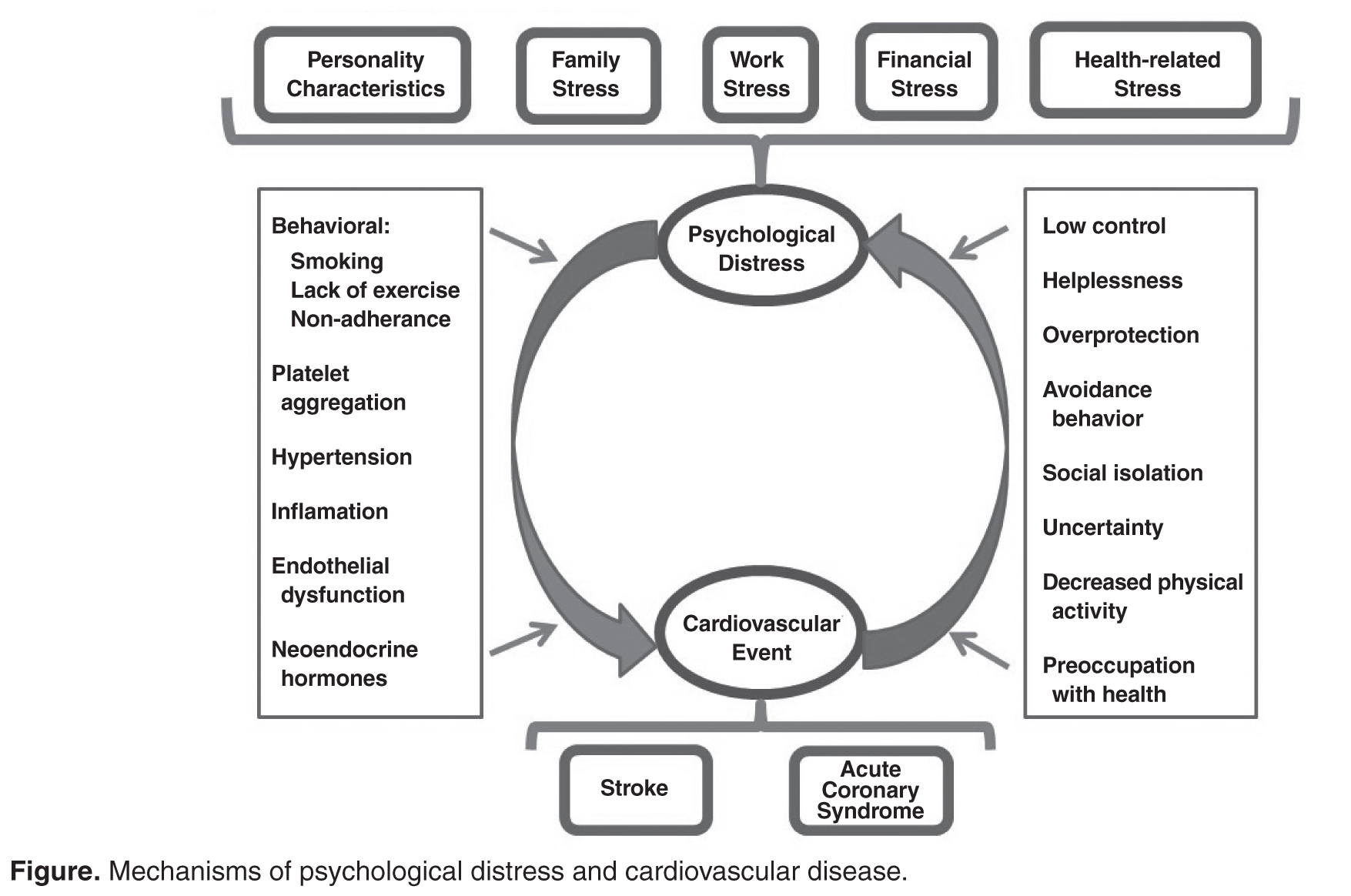
Psychological distress is created by a number of factors ( Figure) such as personality characteristics, family stress, work stress, financial stress, and health-related stress [10–12]. These stressors are thought to create an internal physiological environment that is deleterious to the vascular system due to multiple behavioral [13] and physiological mechanisms [14], which ultimately lead to an acute event such as an acute coronary syndrome (ACS) or stroke. In turn, once a CVD event occurs, multiple psychological, sociological, and behavioral factors perpetuate psychological distress, which together with CVD is responsible for numerous poor outcomes.
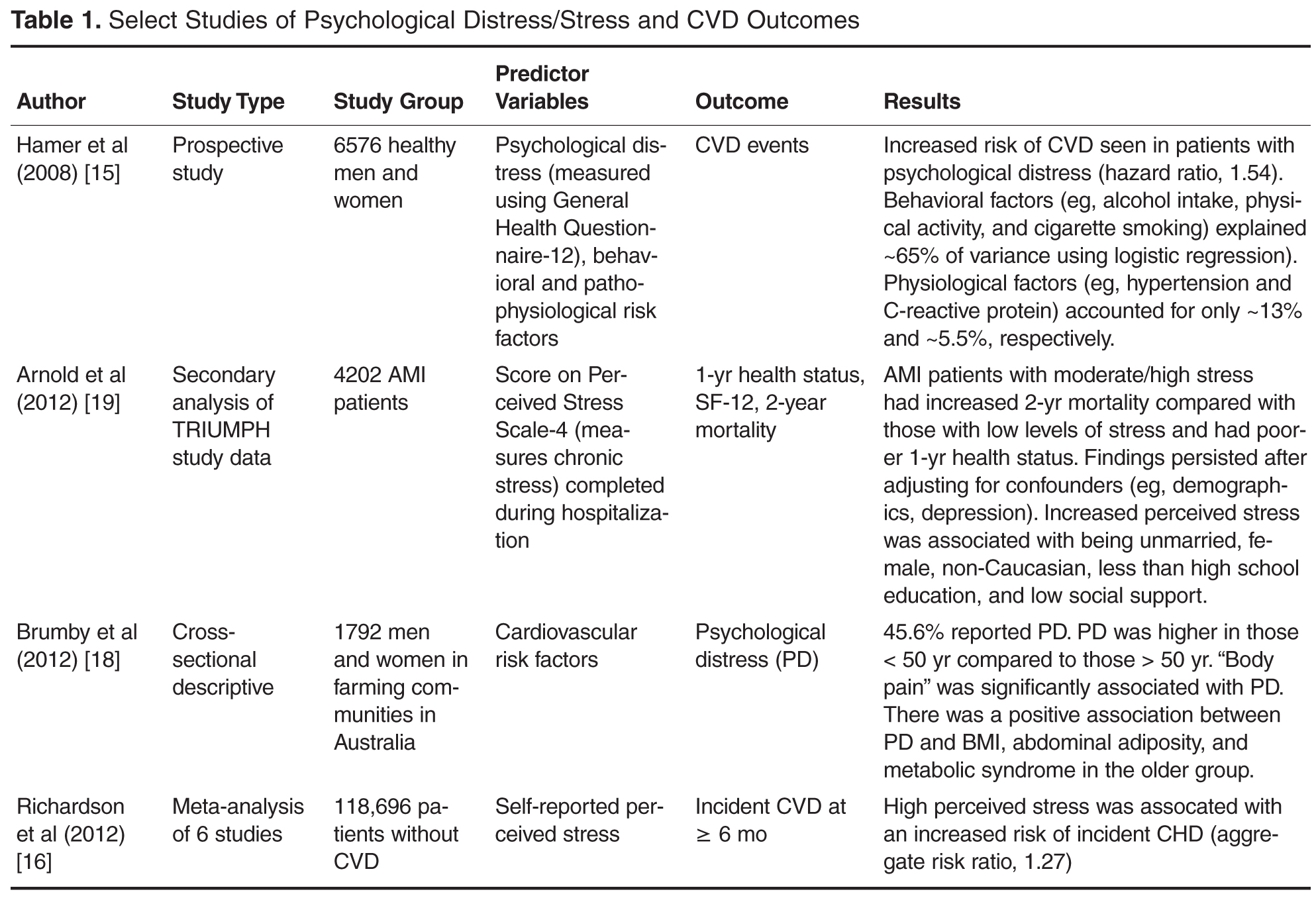
Multiple behavioral (eg, alcohol intake, physical activity, cigarette smoking) and physiologic (eg, body pain, abdominal adiposity, inflammation, hemodynamic disturbances) mechanisms have been identified as likely mediators between the increase in CVD related to psychological distress [15–17]. Large studies and meta-analyses ( Table 1 ) establish that an increased risk and incidence of coronary heart disease (CHD), potentially leading to acute myocardial infarction (AMI), exists in patients with perceived stress [16], stress [17], and psychological distress [15,18]. A meta-analysis equated the increase incidence of coronary heart disease associated with perceived stress to increases in blood pressure, low-density lipoproteins, and smoking [16]. Chronic perceived stress was reported by more than one-third of discharged post-myocardial infarction patients in a secondary analysis of the TRIUMPH (Translational Research Investigating Underlying disparities in acute Myocardial infarction Patients’ Health status) study, with half of those describing depressive symptoms [19]. The chronic perceived stress was independently associated with an increase in post-AMI mortality.
Psychological Distress Disorders Related to CVD
Depression, anxiety, and post-traumatic stress disorder (PTSD) are the 3 most common psychological distress disorders related to CVD [20]. Cardiac disease and depression has been most commonly studied. In stroke, the science is not as well evolved due to greater heterogeneity of study samples and outcome measures.
Depression
Dysphoria (feeling blue), anhedonia (inability to experience joy in otherwise enjoyable activities), insomnia or hypersomnia, fatigue or loss of energy, increased guilt or worthlessness, decreased concentration, appetite change with significant weight loss or gain, psychomotor retardation or agitation, and suicidal ideation are the symptoms of depression [21]. These symptoms exist on a continuum, ranging from mild symptoms with short duration and limited functional impairment to major depression. Importantly, among otherwise healthy individuals, even minor depressive symptoms have been significantly associated with increased incidence of coronary disease [22].
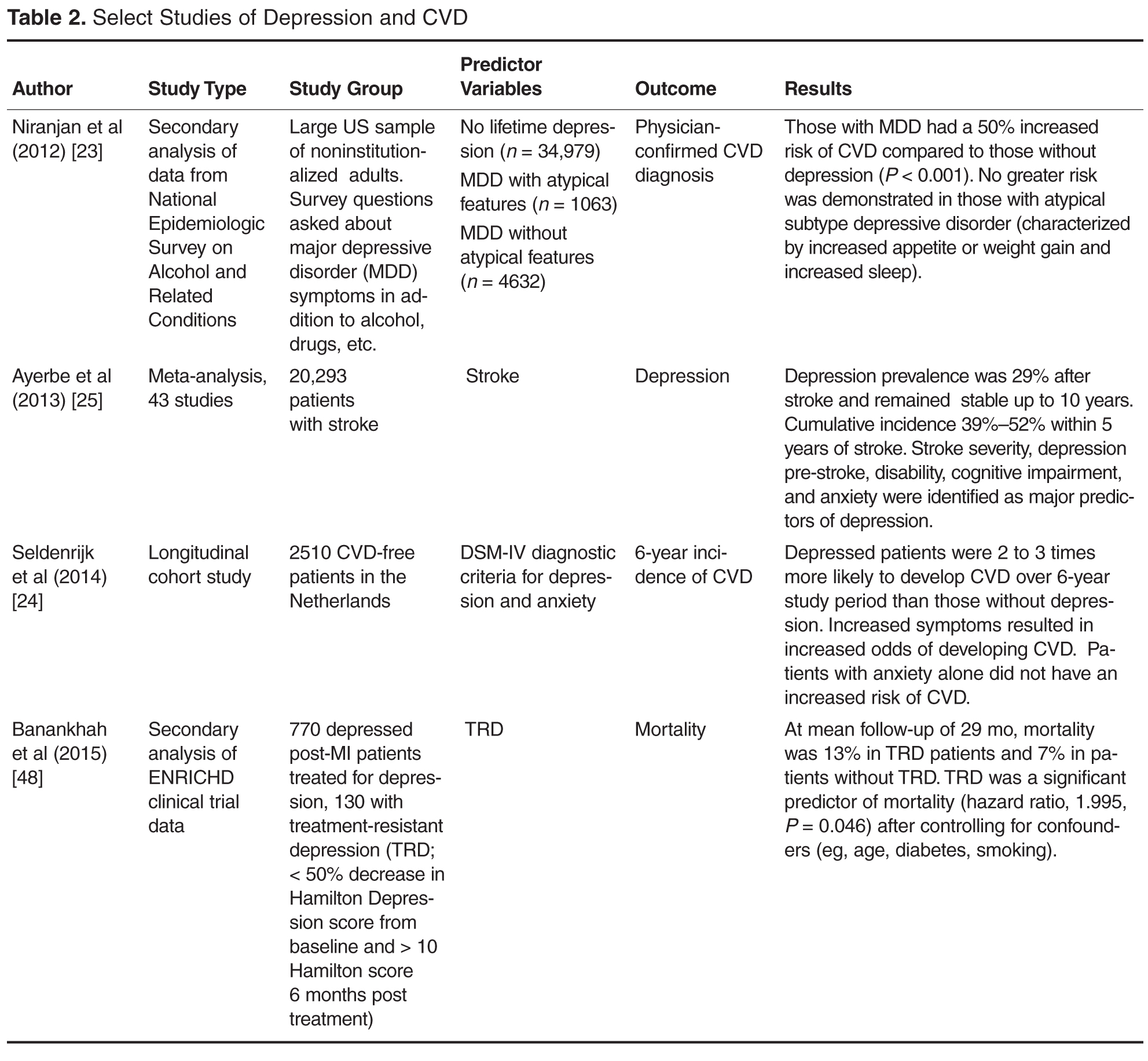
The breadth of research on depression and CVD is demonstrated by the selected large studies and meta-analyses presented in Table 2 . In a large study of 43,093 individuals in the National Epidemiologic Survey on Alcohol and Related Conditions, major depressive disorder was shown to increase the odds of any cardiovascular disorder by 50% ( P < 0.001) [23]. In the longitudinal Netherlands Study of Depression and Anxiety, a 2 to 3 times greater likelihood of developing CVD over a 6-year period was reported in patients with depression compared to those without depression [24] . These recent findings are consistent with the data in the literature presented over the past 2 decades [13] .