Early Parkinsonism: Distinguishing Idiopathic Parkinson’s Disease from Other Syndromes
Journal of Clinical Outcomes Management. 2015 June;22(6)
References
Normal pressure hydrocephalus (NPH) refers to chronic communicating hydrocephalus with adult onset. The classic clinical triad of NPH includes cognitive impairment, urinary incontinence, and gait disturbance in the absence of signs of increased intracranial pressure such as papilledema. NPH can present with motor signs similar to those found in vascular parkinsonism, possibly due to the close proximity of basal ganglia structures to the ventricular system [52]. The gait of NPH typically shows a decrease in step height and foot clearance as well as a decrease in walking speed. This is often referred to as a “magnetic gait.” In contrast to Parkinson’s disease patients, the gait disturbance in NPH does not improve with visual cues or dopaminergic therapy [53]. Dementia also occurs early on in the course of NPH and is mostly characterized by apathy, forgetfulness, and impaired recall. Urinary incontinence and urgency is a later finding of the disease in contrast to IPD in which urinary dysfunction is often an early nonmotor symptom. MRI and CT scans of the brain reveal enlarged ventricles (out of proportion to surrounding cerebral atrophy if present) and should be followed by a diagnostic high volume lumbar puncture. Clinical improvement following lumbar puncture is supportive of the diagnosis of NPH and helps to identify patients who may benefit from ventriculoperitoneal shunting [54].
Essential tremor (ET) is characterized by postural and action tremors, rather than resting tremors, though some ET patients can have co-existing resting tremors. Though it is usually bilateral, it is often asymmetric, adding to the potential for diagnostic confusion with IPD. It typically has a higher frequency than the tremor of IPD. The absence of rigidity, bradykinesia, postural and gait disturbances and no response to dopaminergic therapy help distinguish it further from IPD [55]. There is phenotypic overlap between these two conditions and some patients with IPD have more postural tremor than rest tremor (or even postural tremor with no rest tremor), while some with long-standing essential tremor may go on to develop parkinsonism [56].
The Role of DaTscan in Diagnosing Early Parkinsonism
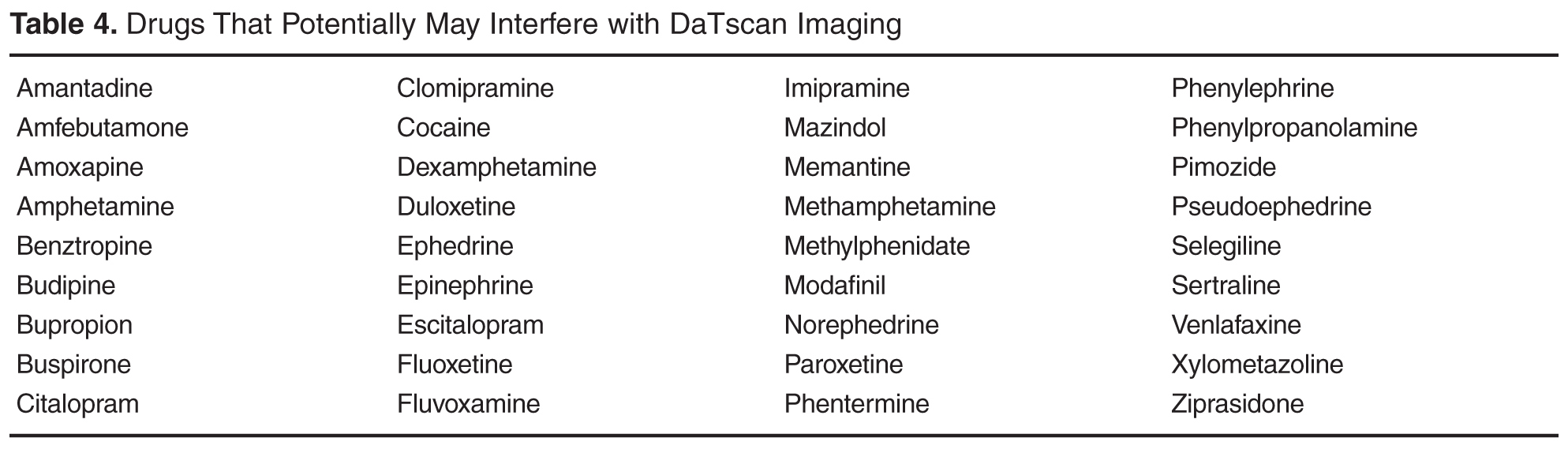
DaTscan is an imaging modality that uses ( 123I)Ioflupane injection with single photon emission computed tomography (SPECT) for detecting dopamine transporters. By binding to the dopamine transporters, a quantitative measure of the transporters in the striatal region of the brain can be obtained [57]. Dopaminergic deficit can be quantified in this manner. While this technology can be extremely useful in certain clinical situations, clinicians should be aware of its limitations. DaTscan cannot differentiate conditions in which there is loss of striatonigral dopaminergic neurons (IPD, PSP, MSA, CBD, LBD), nor can it distinguish between conditions where there is no loss of dopamine neurons (ET, DIP, psychogenic conditions) [58]. In clinical use, these scans are mostly used for differentiation of IPD from essential tremor, and are more often used if tremor is the most prominent symptom (which can make distinguishing between IPD and essential tremor difficult). It is important to mention that drugs that bind to the dopamine transporter with high affinity may interfere with the image, and the impact of dopamine agonists and antagonists on the imaging results has not been established. Drugs that may potentially interfere with DaTscan imaging are listed in Table 4