
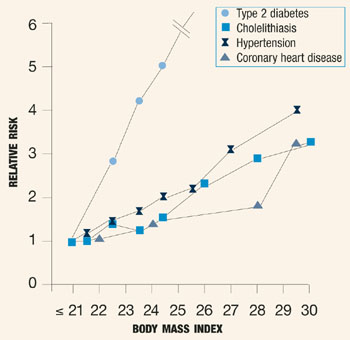
If ever there was a time to convince our patients to change their dietary habits, it is now. The New Year offers the perfect occasion, and a recent study in the New England Journal of Medicine supplies the troubling statistics: Compared with women of normal body weight, obese women have a 20.1 relative risk (RR) of developing type 2 diabetes mellitus. Even women at the high end of the normal range face a RR of 2.67.1 Obesity also has been associated with a three- to fourfold increased risk of hypertension and coronary heart disease (Figure 1). In the United States, only smoking contributes more than obesity to total mortality rates.2
 Source: Willett WC, Dietz WH, Colditz GA. Primary care: guidelines for healthy weight. N Engl J Med. 1999;341:427-434.
Source: Willett WC, Dietz WH, Colditz GA. Primary care: guidelines for healthy weight. N Engl J Med. 1999;341:427-434.
FIGURE 1 Risk of disease relative to BMI
To make matters worse, obesity is rampant, with an age-adjusted prevalence that rose by approximately 30% between 1980 and 1994.3 One way we can help is to encourage a stable body weight tied to height and bone structure. And lest you think your efforts will be in vain, consider this: In a survey of approximately 13,000 obese Americans who had visited their doctor for a check-up in the previous year, those counseled to lose weight were almost 3 times more likely to attempt to do so.4 One way to broach the subject is to explain the body mass index (BMI), an individual’s weight in kilograms divided by the square of her height in meters. A healthy BMI ranges from 18.5 to 24.9 kg/m2, while BMIs equal to or greater than 25 and 30 kg/m2 define overweight and obesity, respectively. The BMI is a significant predictor of risk for coronary heart disease, hypertension, and cholelithiasis and is the single most important predictor of dia-betes.1 Unfortunately, the public has little awareness of the link between obesity and diabetes. That’s where we come in.
We might start by asking: “Did you know you can prevent diabetes by changing your diet?” The patient’s BMI can then be calculated, and a brief discussion of dietary habits can ensue. Women should be counseled to cut down on saturated fats (such as those found in red meat) and trans-fats (partially hydro-genated vegetable oil), as these are clearly associated with an increased risk of coronary heart disease and diabetes.1 In contrast, monounsaturated fats (olive oil) and fats rich in omega-3 fatty acids (vegetable and fish oils) decrease the risk of both coronary heart disease and diabetes.
Women also should be encouraged to cut down on foods with a high glycemic index (refined sugar, white bread, and pizza), which produce large, rapid increases in blood glucose and insulin. Instead, they should focus on carbohydrates with a low glycemic index (whole grains, beans, and vegetables)—also known as complex carbohydrates—which cause slow, minimal increases in glucose and insulin, reducing the risk of diabetes. And here’s more encouragement: A combination of regular exercise, a diet rich in complex carbohydrates and low in trans-fats, and maintenance of a normal BMI is associated with an 87% reduction in the risk of diabetes!1
In counseling patients, clinicians also should be sensitive to the personal and cultural factors that influence eating habits. A middle-aged woman who has consumed a diet heavy in starches and red meat for much of her life cannot be expected to abandon such tastes overnight. In many instances, however, information and encouragement to make incremental changes will achieve the greatest long-term effects.
Whatever the approach, the risks of obesity need to be mentioned regularly. No other intervention may have as great an impact on overall quality of life.