Elizabeth A. Jackson, PharmD, BCPS, BCPP Clinical Pharmacy Specialists–Mental Health Veterans Affairs San Diego Healthcare System San Diego, California
Aila J. Spiegel, PharmD, BCPP Clinical Pharmacy Specialist–Mental Health, Veterans Affairs Central Texas Healthcare System Austin, Texas
Rebecca L. Graham, PharmD, BCPP Clinical Pharmacy Specialists–Mental Health Veterans Affairs San Diego Healthcare System San Diego, California
When to initiate Most treatment guidelines9-17 recommend clozapine only after monotherapy with at least 2 other antipsychotics fails. It is reasonable to add an antipsychotic to clozapine in patients who have shown a partial response to clozapine after a minimum of 3 months. Non-clozapine APP should be considered when:
a patient derives no benefit from clozapine
refuses clozapine
clozapine is contraindicated
APP is initiated to mitigate side effects from another antipsychotic.
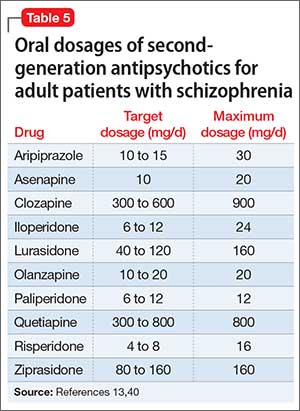
Antipsychotics could take up to 16 weeks to achieve full efficacy,6 therefore, an adequate trial period within the target dosage range is advised for all antipsychotics (Table 5).13,40
Why initiate Based on available data, partial response to maximum recommended dosages of antipsychotic monotherapy, including clozapine, or inability to tolerate higher dosages, provides a reason for initiating APP. Non-clozapine APP generally should be considered only in patients who refuse, cannot tolerate, or do not respond to clozapine. Consider using validated rating scales to track treatment outcomes (ideally, a ≥20% symptomatic reduction on the BPRS or PANSS), although there is no formal guidance regarding their use or benefit in APP.
Summing up APP is a fairly common prescribing practice, even though safety and efficacy data are mixed. The issue of APP has become prevalent enough that regulatory bodies are involved in its monitoring and documentation.41
Clozapine APP, especially with risperidone, has the most substantial evidence to support it. Although APP generally is well tolerated, the overall dearth of conclusive safety and efficacy data indicates that this practice should be reserved for patients who have not responded adequately to monotherapy, including clozapine. Adjunctive aripiprazole could be considered for addressing symptomatic hyperprolactinemia or other metabolic effects caused by other antipsychotics.
An adequate trial as long as 16 weeks is advised before assessing the efficacy of any antipsychotic regimen. If APP provides inadequate response, or if there is no clear indication for APP, consider switching the patient back to monotherapy.42-44
Related Resource
Kontos N, Freudenreich O, Querques J. Reducing polypharmacy: when less is more. Current Psychiatry. 2010;9(3):80.
Disclosures The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.