




Article
Poromatosis in Pregnancy: A Case of 8 Eruptive Poromas in the Third Trimester
The poroid family of neoplasms includes hidroacanthoma simplex, eccrine poroma, dermal duct tumor, and poroid hidradenoma. These benign adnexal...
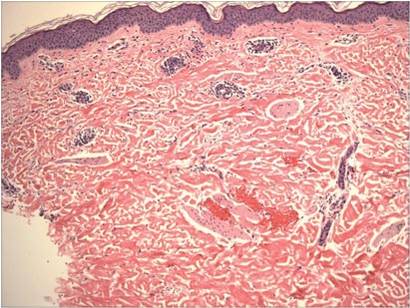
Pruritic urticarial papules and plaques of pregnancy (PUPPP)(also known as polymorphic eruption of pregnancy in Europe) is an intensely pruritic eruption that affects women during the third trimester of pregnancy. Treatment usually is aimed at symptom relief until delivery, as the eruption usually resolves rapidly in the postpartum period. We report the case of a 30-year-old woman who presented 2 weeks postpartum with an intensely pruritic generalized eruption. The eruption started on the abdominal striae within 24 hours of delivery and gradually spread to the buttocks, legs, and arms. Punch biopsy confirmed a diagnosis of PUPPP. Pruritic urticarial papules and plaques of pregnancy presenting in the postpartum period is extremely rare. We present this case for clinical interest and to remind clinicians to keep PUPPP as a consideration in the differential diagnosis when evaluating pruritic eruptions in women who are in the postpartum period.
Practice Points
The poroid family of neoplasms includes hidroacanthoma simplex, eccrine poroma, dermal duct tumor, and poroid hidradenoma. These benign adnexal...

We report the case of a 34-year-old woman who was diagnosed with pemphigus vulgaris (PV) during pregnancy. The patient presented with widespread...