Article

Furuncular Myiasis in 2 American Travelers Returning From Senegal
Furuncular myiasis caused by Cordylobia anthropophaga larvae is commonly seen in Africa but rarely is diagnosed in travelers returning from the...
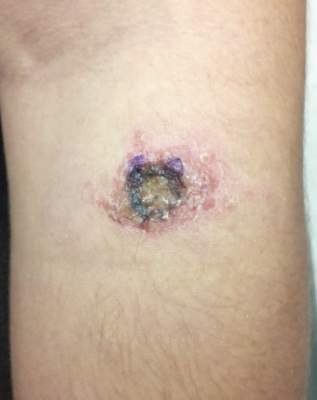
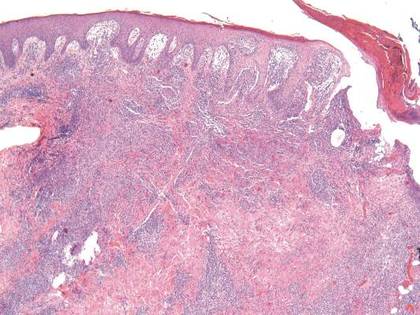
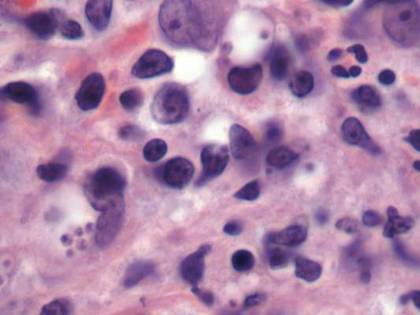
Leishmaniasis describes any of 3 diseases caused by protozoan parasites of the genus Leishmania, the most common of which is cutaneous leishmaniasis. The majority of cutaneous cases occur in Central and South America, the Mediterranean basin, the Middle East, and Central Asia. Most cases diagnosed among nonmilitary personnel in the United States are acquired in Mexico and Central America. Here, we present the case of an American tourist who developed localized cutaneous leishmaniasis 2 weeks after returning from Costa Rica. After undergoing several unsuccessful rounds of empiric antibiotic treatment for a presumed Staphylococcus aureus skin infection, the patient was referred to our dermatology clinic where cutaneous leishmaniasis was diagnosed by tissue biopsy. This case highlights the importance of cutaneous leishmaniasis as an emerging infectious disease that may be misdiagnosed due to its rarity and varied clinical presentation as well as the limited use of tissue biopsy in general practice. We also provide relevant background information on cutaneous leishmaniasis, a rhyming poem, and an illustration in order to promote greater awareness of this disease and assist clinicians with its diagnosis.
Practice Points
Furuncular myiasis caused by Cordylobia anthropophaga larvae is commonly seen in Africa but rarely is diagnosed in travelers returning from the...

Global travel has become ubiquitous for recreational, occupational, educational, humanitarian, and other purposes. For this reason, those who...