Ms. Brankov is from Loma Linda University School of Medicine, California. Drs. Moore, Messana, and Piliang are from the Departments of Dermatology and Pathology, Cleveland Clinic, Ohio.
The authors report no conflict of interest.
Correspondence: Nikoleta Brankov, BS, Loma Linda University School of Medicine, 24570 Stewart St, Loma Linda, CA 92354 (nikoleta.brankov@gmail.com).
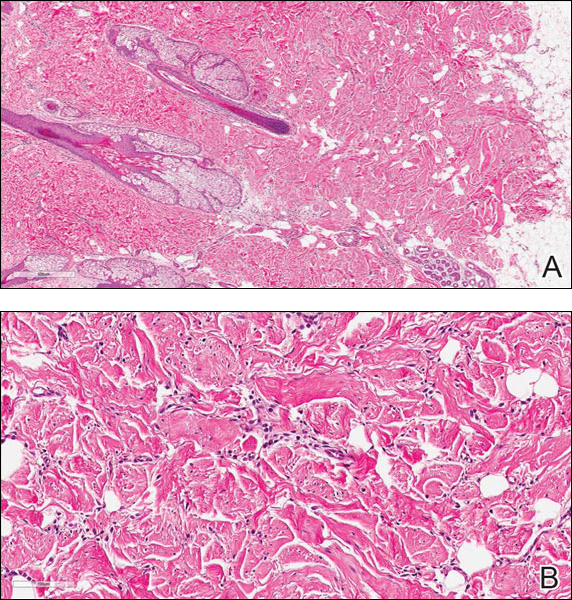
Figure A. H&E, original magnification ×4. Reference bar denotes 500 μm. Figure B. H&E, original magnification ×20. Reference bar denotes 100 μm.
The best diagnosis is:
a. dermatofibroma b. nuchal-type fibroma c. sclerotic fibroma d. solitary fibrous tumor e. spindle cell lipoma
Continue to the next page for the diagnosis >>
References
Nuchal-Type Fibroma
Nuchal-type fibroma (NTF) is a rare benign proliferation of the dermis and subcutis associated with diabetes mellitus and Gardner syndrome.1,2 Forty-four percent of patients with NTF have diabetes mellitus.2 The posterior aspect of the neck is the most frequently affected site, but lesions also may present on the upper back, lumbosacral area, buttocks, and face. Physical examination generally reveals an indurated, asymptomatic, ill-defined, 3-cm or smaller nodule that is hard and white, unencapsulated, and poorly circumscribed.
Histopathologic examination of NTF typically reveals a nodular paucicellular proliferation of thick collagen bundles with inconspicuous fibroblasts, radiation of collagenous septa into the subcutaneous fat, and entrapment of mature adipose tissue and small nerves (quiz image A). Collagen bundles are thickened with entrapment of adipose tissue without increased cellularity (quiz image B). S-100 staining can show the entrapped nerves.
Similar to NTF, sclerotic fibroma is a firm dermal nodule with histologic examination usually demonstrating a paucicellular collagenous tumor. In sclerotic fibromas, the collagen pattern resembles Vincent van Gogh’s painting “The Starry Night” and may be a marker for Cowden disease (Figure 1).3 Solitary fibrous tumors are distinguished by more hypercellular areas, patternless pattern, and staghorn-shaped blood vessels (Figure 2).4 Spindle cell lipoma classically demonstrates a mixture of mature adipocytes and bland spindle cells in a mucinous or fibrous background with thick collagen bundles with no storiform pattern (Figure 3). Some variants of spindle cell lipoma have minimal or no fat.5 All of these conditions have positive immunohistochemical staining for CD34.
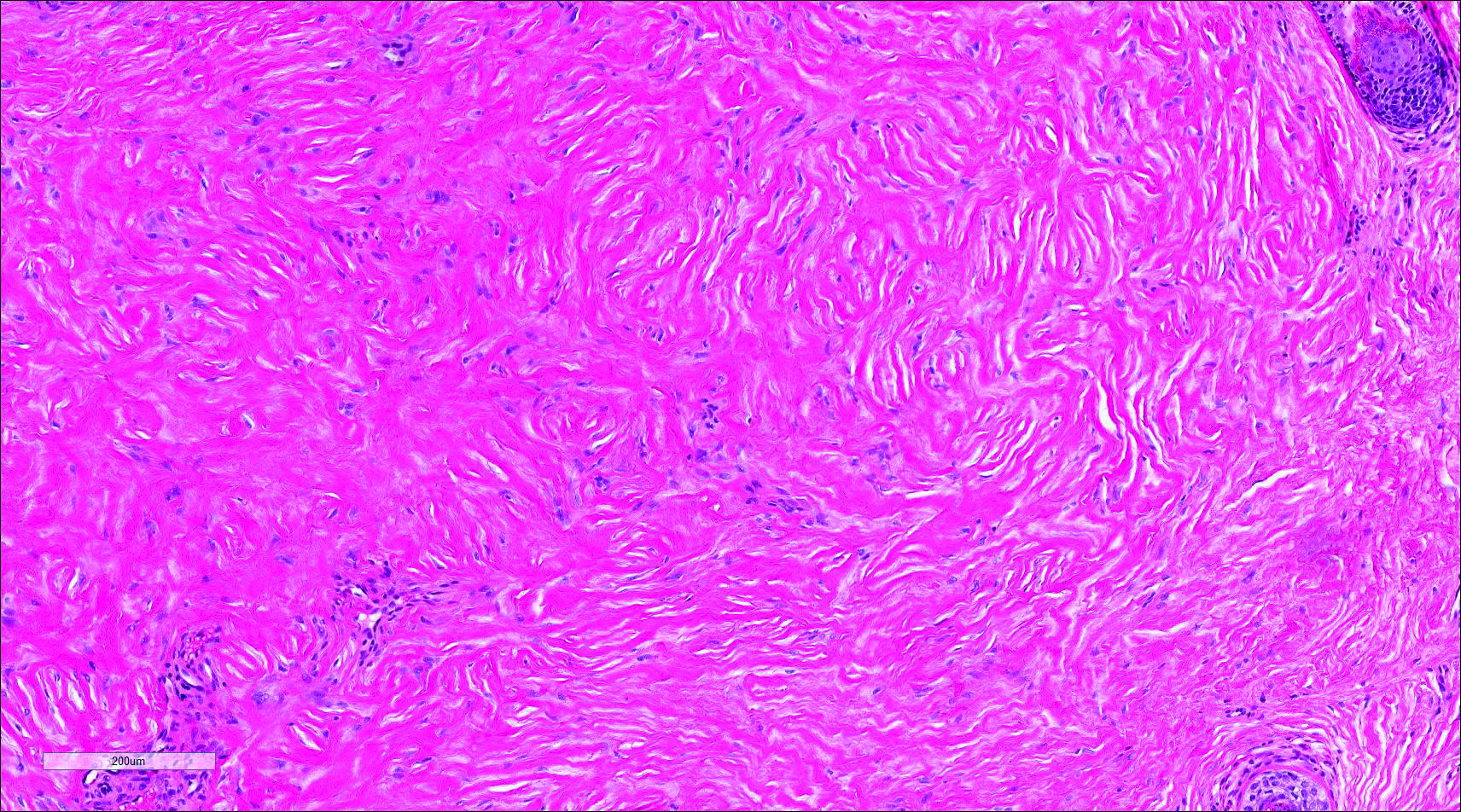
Figure 1. Sclerotic fibroma with a collagen pattern resembling Vincent van Gogh’s painting “The Starry Night” as well as hypocellular areas (H&E, original magnification ×10). Reference bar denotes 200 μm.
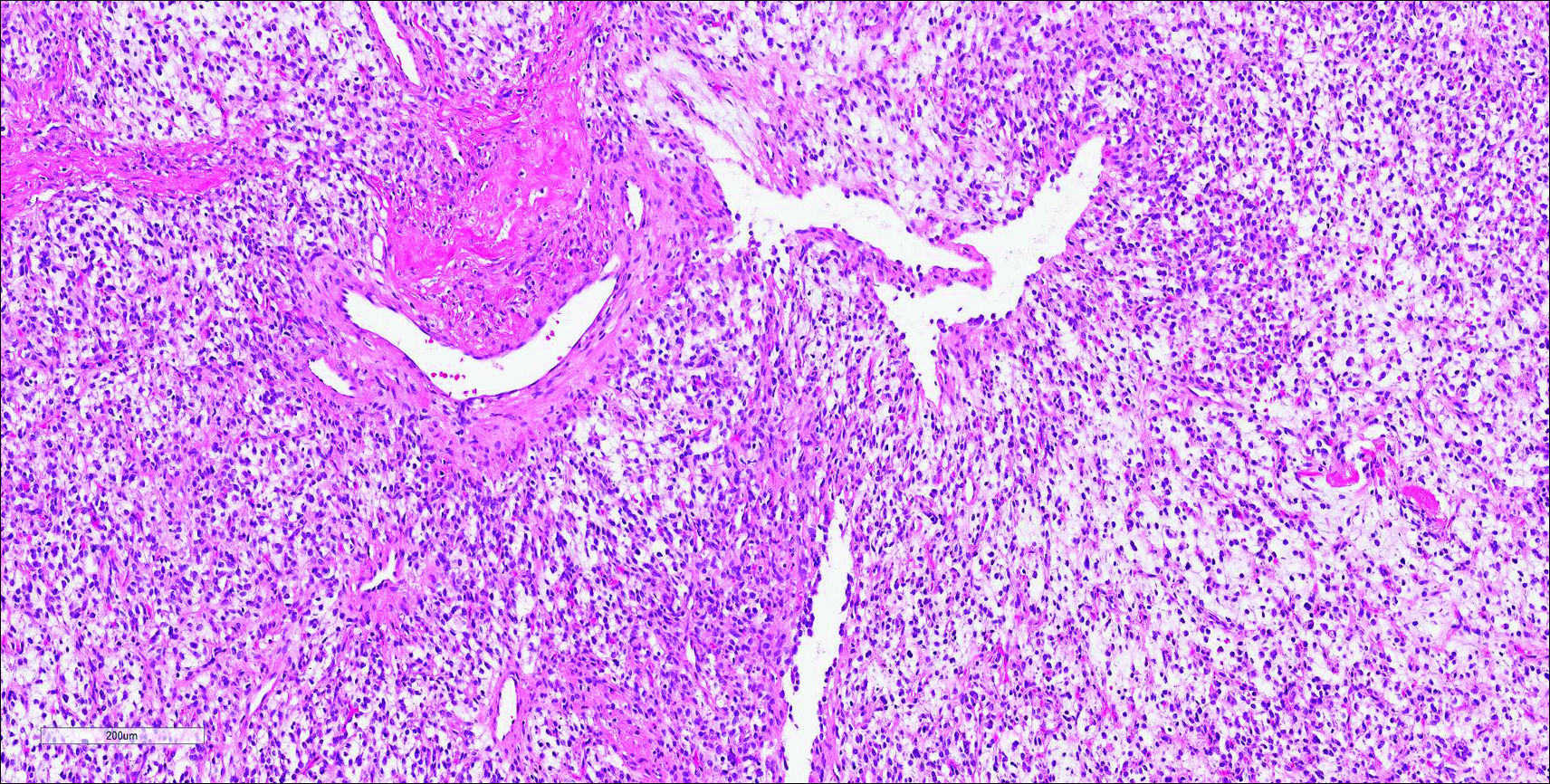
Figure 2. Solitary fibrous tumor with a hemangiopericytomalike branching vascular network, patternless pattern of fascicles, and hypocellular and hypercellular regions separated by hyalinized collagen (H&E, original magnification ×10). Reference bar denotes 200 μm.
Figure 3. Spindle cell lipoma shows adipose tissue with interspersed regions of spindle cells and collagen with areas of ropey collagen bundles (H&E, original magnification ×10). Reference bar denotes 200 μm.
However, dermatofibroma is CD34‒. Dermatofibroma is characterized by an interstitial spindle cell proliferation with a loose storiform pattern, collagen trapping at the outer edges of the tumor, overlying platelike acanthosis, and sometimes follicular induction (Figure 4).
Figure 4. Dermatofibroma with interstitial spindle cell proliferation and collagen trapping (H&E, original magnification ×10). Reference bar denotes 200 μm.
Nuchal-type fibroma also can resemble scleredema. Both lesions can show increased and thickened collagen bundles without notable fibroblast proliferation; the difference is the occurrence of mucin in scleredema. However, incases of late-stage scleredema, mucin is not always demonstrated. Therefore, one can conclude that histologically NTF is closely associated with late-stage scleredema.6