From the Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York.
The authors report no conflict of interest.
Correspondence: Gary Goldenberg, MD, Department of Dermatology, Icahn School of Medicine at Mount Sinai Medical Center, 5 E 98th St, New York, NY 10029 (garygoldenbergmd@gmail.com).
The treatment of palmoplantar hyperhidrosis benefits from regional blocks. Botulinum toxin has been well established as an effective therapy for the condition.19-21 Given the sensitivity of palmoplantar sites, it is valuable to achieve effective analgesia of the region prior to dermal injections ofbotulinum toxin.
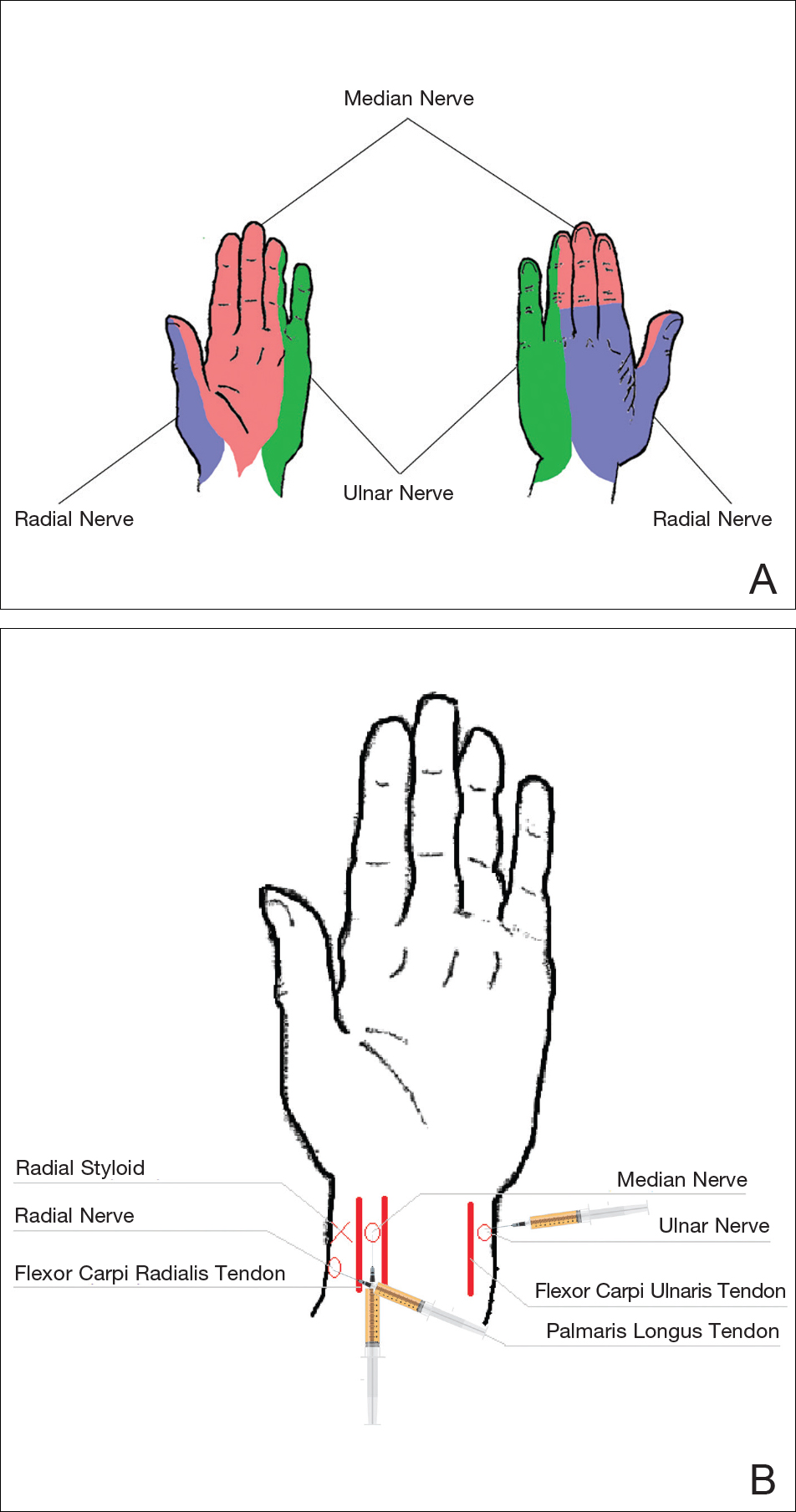
Wrists Sensory innervation of the palm is provided by the median, ulnar, and radial nerves (Figure 2A). At the wrist, the median nerve lies between the tendons of the flexor carpi radialis muscle and the palmaris longus muscle. To facilitate identification of the palmaris longus muscle, instruct the patient to oppose the thumb and little finger while flexing the wrist. The needle should be inserted between the 2 tendons, just proximal to the wrist creases (Figure 2B). Once the fascia is pierced, 3 to 5 mL of anesthetic is injected.
The ulnar nerve is anesthetized between the ulnar artery and the flexor carpi ulnaris muscle. The artery is identified by palpation, and special care should be taken to avoid intra-arterial injection. The needle is directed toward the radial styloid, and 3 to 5 mL of anesthetic is injected roughly 1 cm proximal to the wrist crease (Figure 2B).
Anesthesia of the radial nerve can be considered a field block given the numerous small branches that supply the hand. These branches are reached by injecting anesthetic roughly 2 to 3 cm proximal to the radial styloid with the needle aimed medially and extending the injection dorsally (Figure 2B). A total of 4 to 6 mL of anesthetic is used.
Figure 2. Regional anesthesia for the wrists. Sensory innervation of the hand (A), and injection points for the median, radial, and ulnar nerves (B).
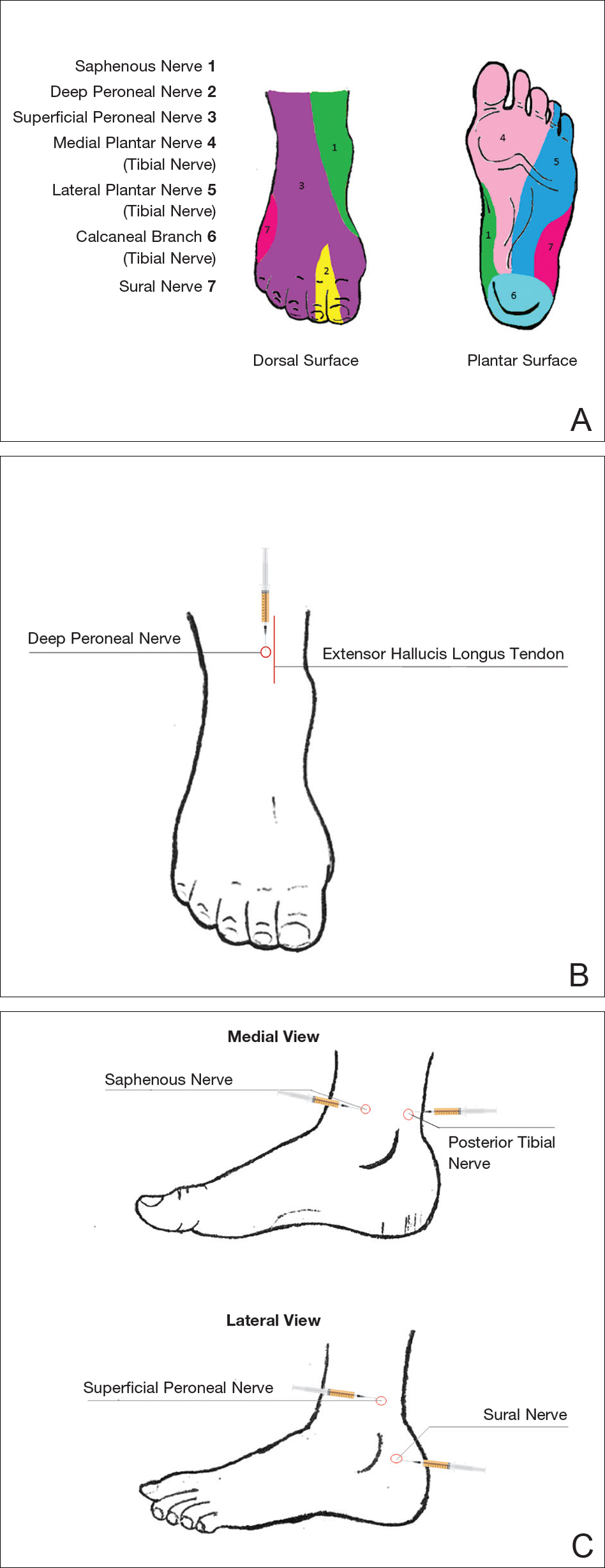
Ankles An ankle block provides anesthesia to the dorsal and plantar surfaces of the foot.22 The region is supplied by the superficial peroneal nerve, deep peroneal nerve, sural nerve, saphenous nerve, and branches of the posterior tibial nerve (Figure 3A).
To anesthetize the deep peroneal nerve, the extensor hallucis longus tendon is first identified on the anterior surface of the ankle through dorsiflexion of the toes; the dorsalis pedis artery runs in close proximity. The injection should be placed lateral to the tendon and artery (Figure 3B). The needle should be inserted until bone is reached, withdrawn slightly, and then 3 to 5 mL of anesthetic should be injected. To block the saphenous nerve, the needle can then be directed superficially toward the medial malleolus, and 3 to 5 mL should be injected in a subcutaneous wheal (Figure 3C). To block the superficial peroneal nerve, the needle should then be directed toward the lateral malleolus, and 3 to 5 mL should be injected in a subcutaneous wheal (Figure 3C).
The posterior tibial nerve is located posterior to the medial malleolus. The dorsalis pedis artery can be palpated near this location. The needle should be inserted posterior to the artery, extending until bone is reached (Figure 3C). The needle is then withdrawn slightly, and 3 to 5 mL of anesthetic is injected. Finally, the sural nerve is anesthetized between the Achilles tendon and the lateral malleolus, using 5 mL of anesthetic to raise a subcutaneous wheal (Figure 3C).
Figure 3. Regional anesthesia for the ankles. Sensory innervation of the foot (A); injection point for the deep peroneal nerve (B); and injection points for the superficial peroneal, sural, saphenous, and posterior tibial nerves (C).
Conclusion
Proper pain management is integral to ensuring a positive experience for cosmetic patients. Enhanced knowledge of local anesthetic techniques allows the clinician to provide for a variety of procedural indications and patient preferences. As anesthetic strategies are continually evolving, it is important for practitioners to remain informed of these developments.