Dr. Morrell is from the Department of Pathology, University of Massachusetts, Worcester. Dr. Mortensen is from Integrated Dermatology of Reno, Nevada. Dr. Langley is from the Department of Dermatology, Loma Linda University, California.
The authors report no conflict of interest.
Correspondence: Travis J. Morrell, MD, MPH, Department of Pathology, University of Massachusetts, One Innovation Dr, Worcester, MA 01605 (travis.morrell@umassmemorial.org).
Amyopathic dermatomyositis (ADM) represents a substantial subset of dermatomyositis (DM). Patients with this symptom of the disorder may present initially to a dermatologist. Amyopathic dermatomyositis shares cutaneous findings with DM and both overlap and differ with respect to other key disease characteristics, including autoantibody profile, associated lung disease, and malignancy risk. Plantar keratoderma is a rare skin finding in DM. We report a case of ADM uniquely marked by the finding of plantar keratoderma, which resolved with oral methotrexate therapy.
Dermatomyositis (DM) can present without muscular weakness as clinically amyopathic dermatomyositis (CADM).
Clinically amyopathic dermatomyositis has cutaneous findings that can mimic other diseases including psoriasis.
Clinically amyopathic dermatomyositis may have similar systemic associations as DM in general, such as an increased risk for malignancies.
Treatments to consider for CADM should include systemic methotrexate.
References
Case Report
A 54-year-old woman presented with a painful pruritic rash on the hands and feet of 7 years’ duration. She reported intermittent joint pain but denied muscle weakness. Physical examination revealed fissured fingertips and heavy scaling of the palms and lateral fingers (Figure 1). Violaceous scaly papules were seen on the distal and proximal interphalangeal joints (Figure 2). A severe plantar keratoderma also was noted (Figure 3). Pink scaly plaques were present on the bilateral elbows and postauricular skin. Diffuse mat telangiectases covered the malar skin. Extensive poikilodermatous skin changes covered approximately 20% of the total body surface area. Salt-and-pepper patches and papules were noted over the bilateral thighs. She reported an uncertain history of recent radiographs of one or both hands, which showed no joint degeneration characteristic of psoriatic arthritis. She previously had been given a diagnosis of psoriasis by an outside dermatologist but was not responding to topical therapy.
Figure 1. Mechanic’s hands in amyopathic dermatomyositis with scaling of the lateral and volar surfaces of the digits as well as the palms.
Figure 2. Gottron papules in amyopathic dermatomyositis with scaling of the dorsal aspects of the interphalangeal joints with an underlying purplish erythema. Surrounding poikilodermatous changes were visible.
Figure 3. Plantar keratoderma with thick, white, hyperkeratotic plaques diffusely covering the sole.
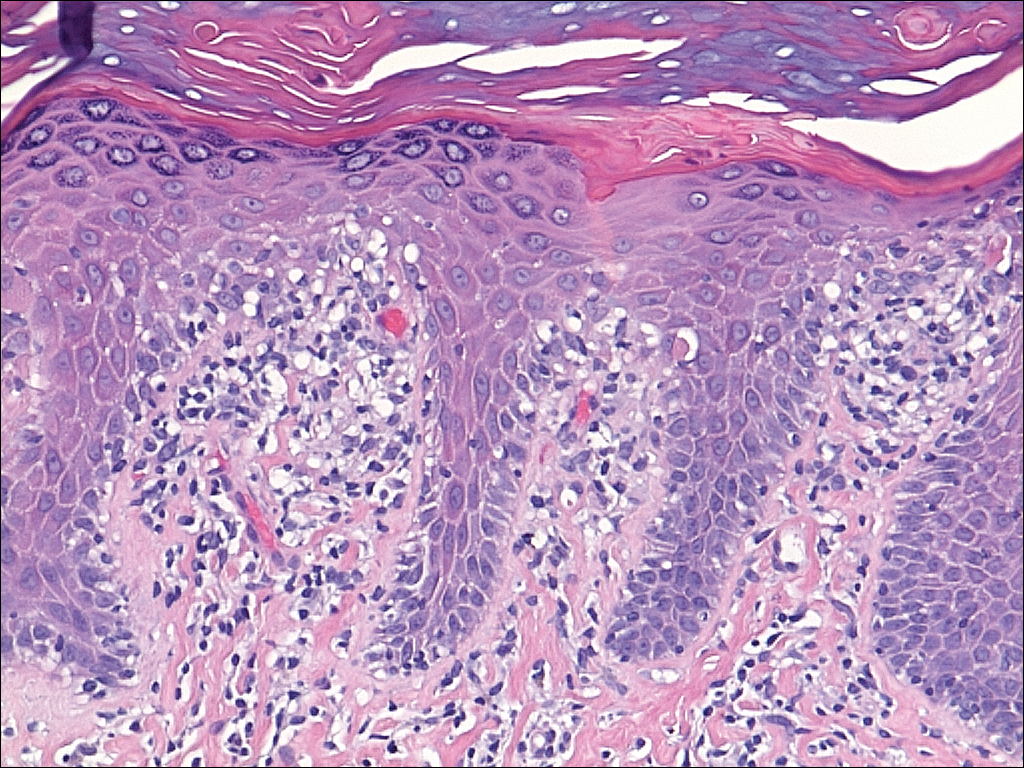
Several skin biopsies showed histologic evidence of dermatomyositis (DM)(Figure 4). Prominent basement thickening also was seen on periodic acid–Schiff staining (not shown). Laboratory workup showed negative antinuclear antibodies and anti–Jo-1, anti-Ku, and anti-Mi2 antibodies. Muscle enzymes including creatinine kinase and aldolase were within reference range. Pelvic ultrasonography and mammography were negative. Pulmonary function tests were unremarkable. High-resolution chest computed tomography (CT) was ordered because of a history of chronic cough; however, no evidence of malignancy or interstitial lung disease was seen. The patient was diagnosed with amyopathic dermatomyositis (ADM). Rheumatology was consulted and initiated oral hydroxychloroquine therapy. After 3 months, the patient’s cutaneous disease did not respond and she reported having headaches associated with this medication; therefore, methotrexate was started. Within 2 months of treatment, full resolution of the plantar keratoderma (Figure 5) and clearance of the scaling/fissuring of the hands as well as the psoriatic-appearing plaques on the elbows was noted.
Figure 4. A shave biopsy of the dorsal aspect of a proximal interphalangeal joint of the right hand with amyopathic dermatomyositis showed psoriasiform epidermal hyperplasia, a smudged dermoepidermal interface, and vacuolar alterations of basal layer (H&E, original magnification ×200).
Figure 5. Plantar keratoderma resolved after 2 months of treatment with oral methotrexate.