Drs. Rutt and Reed are from Lehigh Valley Health Network, Allentown, Pennsylvania. Dr. Liu is from Principle Diagnostics, Bethlehem, Pennsylvania. Dr. Richard is from Johns Hopkins Department of Dermatology, Lutherville, Maryland. Dr. Purcell is from Advanced Dermatology Associates LTD, Allentown.
The authors report no conflict of interest.
Correspondence: Veronica L. Rutt, DO, Lehigh Valley Health Network, 1259 S Cedar Crest Blvd, Ste 100, Allentown, PA 18103 (Veronica.Rutt.DO@gmail.com).
Photosensitive atopic dermatitis (AD) is a rare disease entity that many physicians are not familiar with, thus it often is misdiagnosed. It can be life altering, as patients often strictly avoid the sun and may only leave the house at night. Effective treatments are available, and therefore diagnosis is key to improve quality of life for these patients. We describe a case of photosensitive AD exacerbated by UVB exposure. The diagnosis was made with phototesting, and the patient was able to begin treatment with narrowband UVB (NB-UVB) hardening while on immunosuppression. The literature on photosensitive AD is limited, and this entity typically is not found in the main dermatology textbooks. Our case emphasizes the diagnostic problems and complexity of photosensitive AD. Histopathologic findings are nonspecific. A thorough history and physical examination can provide the necessary clues for further workup. Phototesting should be performed to confirm the diagnosis and evaluate the degree of sensitivity to UV light and the specific wavelength eliciting the cutaneous response. Photoprovocation and photopatch testing also can be useful to confirm the diagnosis.
Photosensitive atopic dermatitis (AD) is rare but should be considered in patients with uncontrolled AD with a rash on sun-exposed skin.
A thorough history and physical examination of these patients can provide the necessary clues for further workup.
Phototesting should be performed to confirm the diagnosis and evaluate the degree of sensitivity to UV light and the specific wavelength eliciting the cutaneous response.
Photoprovocation and photopatch testing also can be useful to confirm the diagnosis.
References
Atopic dermatitis (AD) is the most common inflammatory skin condition, affecting approximately 15% to 20% of the global population.1,2 Atopic dermatitis is characterized by a chronic relapsing dermatitis with pruritus, often beginning in infancy or childhood. Atopic dermatitis is caused by a defect in epidermal barrier function, which results in increased transepidermal water loss.1 The criteria for AD include a pruritic skin condition plus 3 or more of the following: history of involvement of the skin creases, history of asthma or hay fever, history of AD in a first-degree relative (in children), 1-year history of generally dry skin, visible flexural eczema, and an age of onset of less than 2 years. Adults with AD frequently present with hand or facial dermatitis.1
UV light therapies including narrowband UVB (NB-UVB), UVA1, and psoralen plus UVA (PUVA) have all been used as effective treatments of AD.3,4 UV light is beneficial for AD patients due to its immunomodulatory effects, thickening of the stratum corneum, and the reduction of Staphylococcus aureus in the skin.2 Most patients with AD improve with light therapy; however, it is estimated that 1% to 3% of patients with AD will experience a paradoxical worsening of their AD after exposure to UV light.2,5 This condition is referred to as photosensitive AD and is characterized by a photodistributed rash in patients who fulfill the criteria of AD. Photosensitive AD has a female predominance and generally affects patients with late-onset disease with development of AD after puberty.2,5 The pathogenesis for the development of photosensitivity in patients with AD who previously tolerated exposure to sunlight is unknown.5 We describe a case of photosensitive AD exacerbated by UVB exposure.
Case Report
A 55-year-old Asian woman presented for evaluation of a rash on the head, neck, and arms. She reported that she had developed a pruritic rash with edema after sun exposure at 16 years of age. Since then, the rash has been intermittent and completely resolved at times with periods of decreased sun exposure; however, the rash recently had been persistent and worsening despite practicing strict sun protection with daily sunscreen application, protective clothing, and sun avoidance. She was not taking systemic medications or supplements at the time but was applying high-potency topical corticosteroids and calcineurin inhibitors with minimal improvement under the care of a dermatologist.
On physical examination the patient had thin, well-demarcated, erythematous papules and plaques with scaling, primarily on sun-exposed skin on the forehead (Figure 1A), cheeks (Figure 1B), eyelids, upper lip, neck (Figures 1B and 1C), upper chest (Figure 1C), and dorsal aspect of the hands, with excoriated pink papules on the forearms, shoulders, and back. A punch biopsy of the right neck showed spongiotic dermatitis with a perivascular lymphohistiocytic infiltrate (Figure 2). Further workup was pursued including complete blood cell count, comprehensive metabolic profile, liver function panel, Sjögren syndrome antigen A/Sjögren syndrome antigen B test, antinuclear antibody test, human immunodeficiency virus 1/2 antigen/antibody test, hepatitis panel, and mycobacterium tuberculosis test, which were all within reference range. Photodermatosis was suspected and she underwent phototesting including UVA, NB-UVB, and visible light. Phototesting confirmed she had a UVB photosensitivity with a markedly decreased minimal erythema dose (MED) to NB-UVB. The MED to NB-UVB was positive at 24 hours to all tested sites, the lowest of which was 0.135 J/cm2. Eczematous changes began to develop at day 6 at doses of 0.945 and 1.080 J/cm2. The patient also underwent visible light testing, which was negative. The patient was patch tested for multiple standardized agents as well as personal products, all of which were negative. Subsequent photopatch testing revealed a slightly positive reaction to benzophenone 4, a common ingredient in sunscreens.
Figure 1. Photosensitive atopic dermatitis on the face (A and B), neck (B and C), and upper chest (C) showing thin erythematous papules and plaques with scaling.
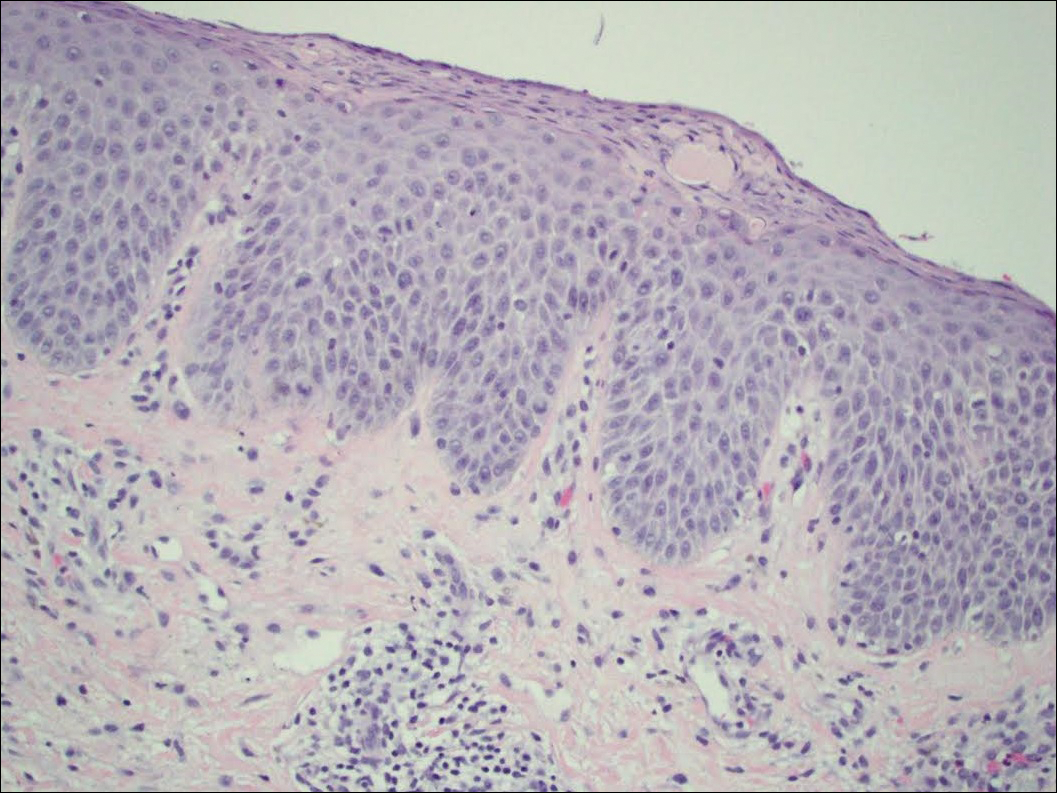
Figure 2. Biopsy of the right neck showed spongiosis, mild uneven psoriasiform hyperplasia, and a superficial perivascular infiltrate of lymphocytes with eosinophils (H&E, original magnification ×40).
The patient was then started on mycophenolate mofetil and prednisone. Repeat MED testing to NB-UVB was performed. Her repeat MED to NB-UVB was determined to be 0.405 J/cm2, and hardening commenced at 3 times per week at 70% of the MED (0.2835 J/cm2). She began to flare and develop an eczematous reaction, thus the dose was decreased to 50% of the MED (0.2025 J/cm2), which she tolerated.