Dr. Pilkington currently is from Azeal Dermatology Institute, Boulder, Colorado. Dr. Pilkington was from and Drs. McKinley and Miller are from the Nova Southeastern College of Osteopathic Medicine, Largo Medical Center, Florida.
Correspondence: Stacey Pilkington, DO, Azeal Dermatology Institute, 5365 Spine Rd, Ste C, Boulder, CO 80301 (staceyseastrom@gmail.com).
Nevoid basal cell carcinoma syndrome (NBCCS) is a rare, autosomal-dominant, cancer-predisposing, multisystem disorder. The clinical manifestations of NBCCS include multiple basal cell carcinomas (BCCs), odontogenic keratocysts, palmar or plantar pits, and calcification of the falx cerebri. We present a case of an 11-year-old boy with Fitzpatrick skin type V who presented with multiple facial lesions and a history of maxillary keratocysts. Skin biopsy was consistent with pigmented BCC of the right nasolabial fold. Further clinical workup revealed multiple pigmented BCCs, palmoplantar pits, and calcification of the tentorium. Genetic testing revealed a heterozygous mutation in the patched 1 gene, PTCH1, consistent with NBCCS. This case highlights the treatment considerations in pediatric cases of NBCCS in Fitzpatrick skin type V patients.
Nevoid basal cell carcinoma syndrome (NBCCS) is a multisystem disorder that requires close monitoring under multidisciplinary care.
The clinical manifestations of NBCCS include multiple basal cell carcinomas, odontogenic keratocysts, palmar or plantar pits, and calcification of the falx cerebri.
References
In 1960, Gorlin and Goltz1 first described nevoid basal cell carcinoma syndrome (NBCCS) as a distinct clinical entity with multiple basal cell carcinomas (BCCs), jaw cysts, and bifid ribs. This rare autosomal-dominant genodermatosis has a minimal prevalence of 1 case per 57,000 individuals2 and no sexual predilection.3 Nevoid basal cell carcinoma syndrome is caused by a mutation in the human homolog of a Drosophila gene, patched 1 (PTCH1), which is located on chromosome 9q22.3.4,5 The major clinical diagnostic criteria includes multiple BCCs, odontogenic keratocysts, palmar or plantar pits, ectopic calcification of the falx cerebri, and a family history of NBCCS.6 Basal cell carcinoma formation is affected by both skin pigmentation and sun exposure; 80% of white patients with NBCCS will develop at least 1 BCC compared to only 40% of black patients with NBCCS.7 Goldstein et al8 postulated that this disparity is associated with increased skin pigmentation providing UV radiation protection, thus decreasing the tumor burden. We report a case of an 11-year-old black boy with NBCCS to highlight the treatment considerations in pediatric cases of NBCCS.
Case Report
An 11-year-old boy with Fitzpatrick skin type V presented with a history of multiple facial lesions after undergoing excision of large keratocysts from the right maxilla, left maxilla, and right mandible. Physical examination revealed multiple light to dark brown facial papules (Figure 1), palmar and plantar pitting (Figure 2), and frontal bossing.
Figure 1. Multiple light to dark brown papules located at the nasolabial sulcus.
Figure 2. Palmar (A) and plantar (B) pitting.
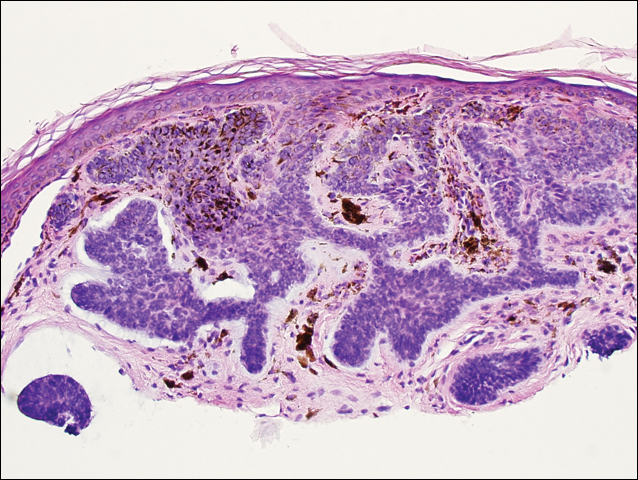
He was previously diagnosed with autism and his surgical history was notable only for excision of the keratocysts. The patient was not taking any medications and did not have any drug allergies. There was no maternal family history of skin cancer or related syndromes; his paternal family history was unknown. A shave biopsy was performed on a facial papule from the right nasolabial fold. Histopathologic evaluation revealed findings consistent with a pigmented nodular BCC (Figure 3). The patient was subsequently sent for magnetic resonance imaging of the brain, which demonstrated calcifications along the tentorium. Genetic consultation confirmed a heterozygous mutation of the PTCH1 gene.
Figure 3. Histopathologic evaluation demonstrated aggregates of pigmented basaloid cells, peripheral palisading, and retraction consistent with a pigmented basal cell carcinoma (H&E, original magnification ×10).
Over the next 12 months, the patient had multiple biopsy-proven pigmented BCCs. Initial management of these carcinomas located on cosmetically sensitive areas, including the upper eyelid and penis, were excised by a pediatric plastic surgeon. A truncal carcinoma was treated with electrodesiccation and curettage, which resulted in keloid formation. Early suspicious lesions were treated with imiquimod cream 5% 5 times weekly in combination with the prophylactic use of tretinoin cream 0.1%. Despite this treatment regimen, the patient continued to demonstrate multiple small clinical pigmented BCCs along the malar surfaces of the cheeks and dorsum of the nose. The patient’s mother deferred chemoprevention with an oral retinoid due to the extensive side-effect profile and long-term necessity of administration.
Management also encompassed BCC surveillance every 4 months; annual digital panorex of the jaw; routine dental screening; routine developmental screening; annual follow-up with a geneticist to ensure multidisciplinary care; and annual vision, hearing, and speech-screening examinations. Strict sun-protective measures were encouraged, including wearing a hat during physical education class.