During her dermatology residency at Yale University in the late 1980s, Tina S. Alster, MD, met a 44-year-old woman who changed the trajectory of her professional career.
 Courtesy Dr. Tina S. Alster
Courtesy Dr. Tina S. Alster
Dr. Tina S. Alster purchased the fourth pulsed dye laser ever to be manufactured. It was originally named SPTL-1, for selective photothermolysis-1. This photo was taken in late 1990 when Dr. Alster opened her practice.
During her clinic visit, the woman explained that she always wore heavy facial makeup to hide her port-wine stain birthmark – a vascular malformation that she kept secret from her husband and teenage son. “She was very good about covering it,” recalled Dr. Alster, who is the founding director of the Washington Institute of Dermatologic Laser Surgery and clinical professor of dermatology at Georgetown University, Washington. “She removed a small amount of makeup for me so I could take a look at it. I had just finished reading an article about using a laser for birthmarks; it had just been published. I told her, ‘There’s something new; we don’t have it at Yale, but I read about treatment that could hone in on birthmarks.’ I promised her I would find out more details.”
A few days later, Dr. Alster pored through stacks of medical journals at Yale’s library and relocated the article she’d seen by first author Oon Tian Tan, MD, PhD, of the department of dermatology at Boston University Medical Center. It described use of the flashpump-pulsed tunable dye laser to treat port-wine stains in 35 children (N Engl J Med. 1989;320:416-21). After giving the article a more thorough read, Dr. Alster became so intrigued by the technology it described that she moved to Boston the following year for a dermatology fellowship with Dr. Tan and joined the ranks of early clinicians who used lasers for treating port-wine stains and other dermatologic conditions.
“That was at a time when there were only a handful of pulsed dye lasers in the world, and the first time I used it was when I went to Boston,” she said. “It was life-changing. You think, ‘Isn’t this great for children with port-wine stains.’ Your heart breaks for them, but I also felt compassion for adults who had suffered a lifetime of stares, including the woman who propelled me to look into this. She ended up coming to Boston during my fellowship and had her birthmark removed, so I changed her life, but she changed mine as well.”
The real credit for that series of events, Dr. Alster continued, belongs to John A. Parrish, MD, and R. Rox Anderson, MD, who in 1983 published the concept of selective photothermolysis, a seminal work that shifted the paradigm for how lasers and other light sources are designed for skin diseases and conditions (Science. 1983 Apr 29;220(4596):524-7). The first pulsed dye laser was built on this concept, an approach that minimized or eliminated the unwanted tissue damage and significant scarring that impeded therapeutic use of laser energy for port-wine stains and other lesions prior to that time. “Lasers that were built subsequent to that seminal paper focused our attention on building lasers that were specific for treatment of certain skin conditions,” Dr. Alster said. “Selective photothermolysis catapulted not only our understanding of how lasers interact with the skin, but allowed us to identify things in the skin that we could potentially target with this new laser technology, and to build laser systems that were specific to those purposes.”
In the late 1970s, Dr. Parrish, who played a key role in making psoralens plus ultraviolet A safe and effective for patients with severe psoriasis, turned his attention to studying lasers in his lab at Harvard Medical School. He hired R. Rox Anderson, a recent graduate of the Massachusetts Institute of Technology, as a technician. “Rox then got interested in medicine and went to medical school at Harvard, got interested in dermatology, and then worked in my lab a little bit more,” said Dr. Parrish, who founded the Wellman Center for Photomedicine at Massachusetts General Hospital, Boston.
“Rox was interested in port-wine stains because of his rotation through pediatrics and was theorizing about how lasers could improve port-wine stains and hemangiomas. I think he first thought of that through the physics of what would be needed. He was thinking, ‘What are these hemangiomas under the microscope? What does the target look like, and what do you need to do to promote healing without scarring? You would have to be able to heat for this duration and this time and at this wavelength.’ He matched the physics of lasers with the pathophysiology of port-wine stains, and together we figured out how to deliver the right energy at the right wavelength at the right time. In fact, at the time, there was no ideal laser. We had to convince a laser manufacturer to build a tunable dye laser, which is what we ended up using around the specifications that we wanted for this treatment.”
Prior to the theory of selective photothermolysis, lasers were a blunt instrument. “They would target the skin but you wouldn’t just selectively target something; you’d get a result you didn’t want,” said Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital.
 Courtesy Dr. Tina S. Alster
Courtesy Dr. Tina S. Alster
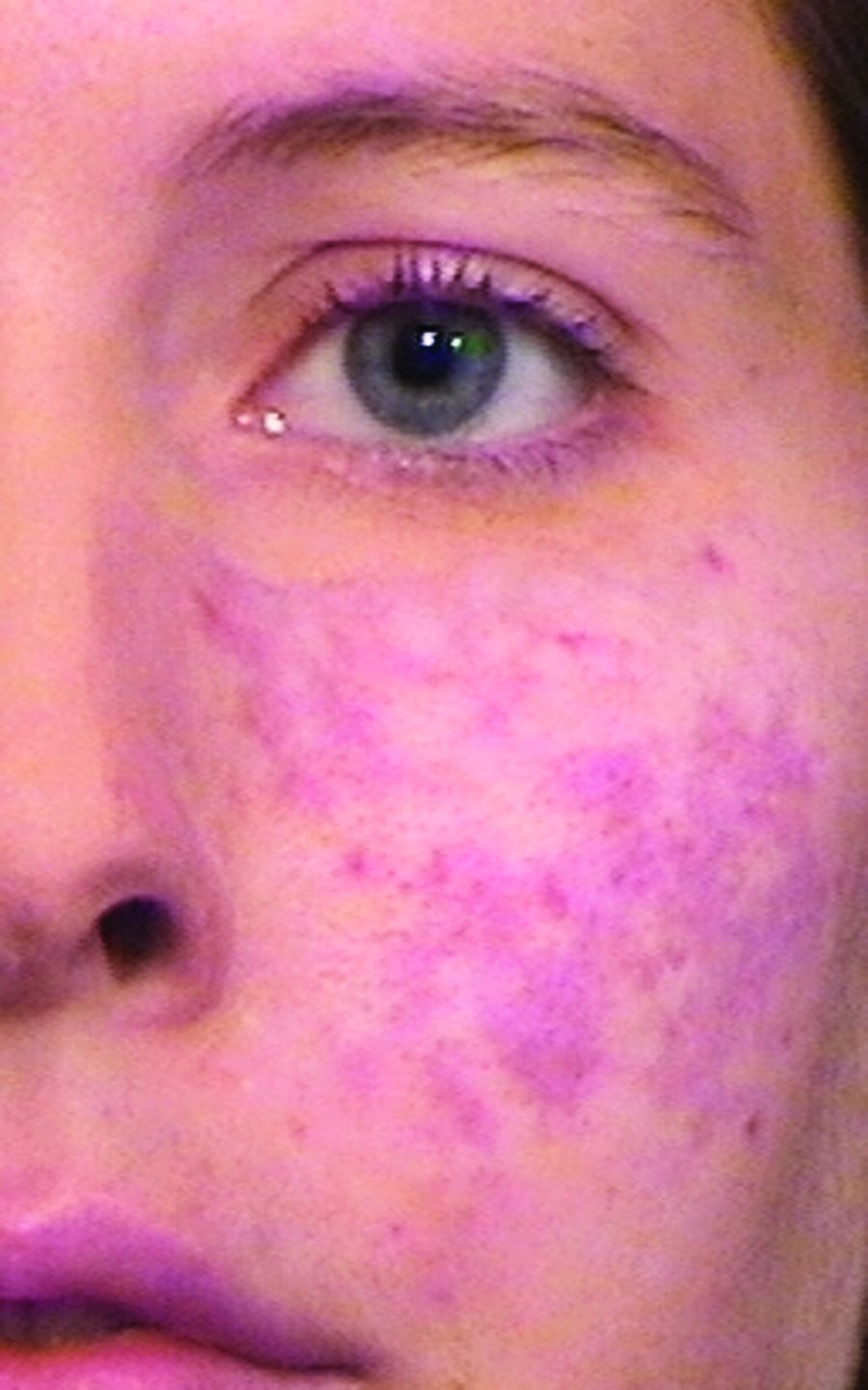
In the early 1990s, this patient presented to Dr. Tina S. Alster with scarring of her port-wine stain that had been previously treated with the argon laser.
Once pulsed dye lasers that incorporated principles of selective photothermolysis hit the marketplace, clinicians could treat and improve port-wine stains without scarring the skin. They could even improve scarring from port-wine stains that had been previously treated with the argon laser, the subject of early published work by Dr. Alster (Lasers Surg Med. 1993;13[3]:368-73). “When we treated port-wine stains with the pulsed dye laser on top of the argon laser scars, we observed that the scars were looking better,” Dr. Alster said. “From that observation, we were able to demonstrate improvement of a wide range of scars: traumatic and burn scars, surgical scars, acne scars, and scars caused by other lasers. But it all started with the pulsed dye laser for treating port-wine stains that had scars in them.”
 Courtesy Dr. Tina S. Alster
Courtesy Dr. Tina S. Alster
After Dr. Alster performed a series of monthly pulsed dye laser treatments, marked improvement of the patient's argon laser-induced scarring was observed.
, which enabled the user to deliver even shorter pulse widths in the nanosecond domain. “That changed tattoo treatment,” said Dr. Avram, who is also a past president of the American Society for Laser Medicine and Surgery. “Prior to that, for tattoos and brown spots you would use ablative lasers like CO2 or dermabrasion. They would cause scarring and not really get rid of the tattoo ink or the brown spots. With the Q-switched nanosecond lasers and the picosecond lasers, which came about 15 years later, you had the ability to remove spots with a week of down time, and [they worked] for things like Nevus of Ota, where someone has a disfiguring blue-brown discoloration of their cheek. There’s no surgical treatment for that whatsoever. It’s not like you can take it out.”
Another key advancement was the introduction of “scanning” technology in the early 1990s for CO2 and erbium YAG lasers, which enabled precise computerized control of laser beams. Dr. Avram characterized the CO2 laser as “the gold standard for facial rejuvenation, for sun-damaged skin. The downside of CO2 lasers is that they really need to be in skilled hands. There can be serious side effects such as scarring if it’s not done appropriately or there is not appropriate follow-up. The CO2 lasers have been used in fractional modes for scars. I think it’s the best treatment for scars.”
Dr. Anderson and Melanie Grossman, MD, who practices in New York City, developed the ruby laser for hair removal in the 1990s, and today that procedure ranks as the most common laser treatment in medicine, according to Dr. Avram. He described it as “safe and effective in skilled hands,” requiring about six treatments. Indications are for hypertrichosis, hirsutism (sometimes in the setting of polycystic ovary syndrome), pseudofolliculitis barbae, pilonidal cysts, and gender reassignment surgery.
Another game-changing technology developed by Dr. Anderson came in the early 2000s with the Food and Drug Administration clearance of the Fraxel laser, which is based on the concept of fractional photothermolysis. With this technology, “instead of treating skin to a certain depth, you treat a fraction of it, anywhere from 5% to 40% of the skin,” Dr. Avram explained. “You go in deeper, but you leave surrounding viable tissue that is not affected by the laser. That serves as viable tissue to promote healing. The laser goes in deeper but it’s fractional, so there are skip zones in between the lasers that are going into the skin. You can do this with the CO2 and erbium YAG lasers.” Since hitting the marketplace, the FDA has cleared the use of Fraxel for a number of indications, from periorbital wrinkles and acne scars to surgical scars and melasma.
Dr. Parrish predicted that the next frontier for the advancement of lasers in dermatology will involve the treatment of photodamaged skin. “I’m not sure which technology is going to win,” he said.
Dr. Avram anticipates that dermatologic lasers of the future are going to be more effective, safer, and result in less downtime for patients. “I think we are going to be able to treat skin of color more safely and more effectively, and I think we’re going to become much more successful,” he said. “At some point, the standard of care of treatment for skin cancer will involve lasers and light sources. With all the advances that have happened in the last 50 years, sometimes you wonder, are we at a time to pause, or is most of the story behind us? I think that the advances in innovation that are occurring are going to accelerate greatly as we pass the 50th anniversary. In due credit, laser therapy has completely revolutionized the field of dermatology and has completely revolutionized the way we practice medicine. That will only accelerate in the future.”
Dr. Alster emphasized a “safety first” approach to her hopes for the future. “My wish is that we educate people to know that, while lasers have become ubiquitous and we’ve made them safe, they’re still only safe in the right hands,” she said. “There’s not a day that goes by when I don’t have somebody referred to me who’s been mishandled. There’s no reason for that. With proper training, the risk of bad side effects or complications is markedly reduced.”