Newer agents, approaches, and techniques have made sclerotherapy more effective with fewer complications than ever before, whereas the basic goal of this therapy remains the same as it was 100 years ago, according to Dr. Margaret Mann.
Sclerotherapy remains the preferred treatment for spider and reticular veins. And with the recent Food and Drug Administration approval of polidocanol, there has been a resurgence of interest in sclerotherapy, she said at the Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
A successful outcome, however, requires the proper patient and sclerosant selection and concentration based on the size of the vessel to be treated, said Dr. Mann, codirector of dermatologic surgery and chief of clinical services in dermatology at the University of California, Irvine.
Also, because the superficial venous system is an interconnected network, the treatment of leg veins should follow a logical algorithmic approach. Patients with great saphenous vein incompetency or perforator disease, for example, should be treated with endovenous ablation and phlebectomy prior to treatment of their spider veins, she explained, noting that it is a myth that unwanted veins can be treated independently of each other.
"Indeed, treating vessels independently results in higher rates of failure, pigmentation, and matting," she said, explaining that a successful outcome requires that the most proximal point of reflux be recognized and treated.
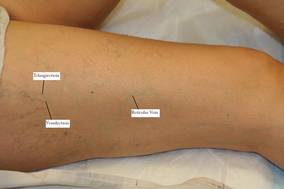
Sclerotherapy is ideal for those with only spider veins and reticular veins, those with minimal or no symptoms, those with a history of successful sclerotherapy, and those with isolated spider veins along the lateral subdermic system.
Consider further testing prior to sclerotherapy in those with significant symptoms, veins that are refractory to multiple sclerotherapy treatments, palpable varicose veins, and/or the presence of corona phlebectasia, as these factors are suggestive of venous insufficiency. Duplex ultrasound for venous reflux should be performed in these patients to help guide treatment, she added.
In those patients for whom sclerotherapy is suitable, Dr. Mann advised using the detergent sclerosants STS (sodium tetradecyl sulfate) or polidocanol when possible for spider and reticular veins, as these are the safest and most efficacious of the FDA-approved sclerosants. Detergent sclerosants have an added advantage, as they can be made into foam.
Foam sclerosants are ideal for larger vessels because the tiny air bubbles trap the sclerosant temporarily, thus increasing contact time between the sclerosant and vein endothelium, and allowing a lower concentration and volume of foam to be used, compared with liquid sclerosant, she explained.
This in turns reduces the risk of complications such as necrosis and pigmentation.
"Match the sclerosant to the caliber of the vessel, and use the lowest effective concentration and volume to optimize outcomes and minimize side effects," she said.
Remember that the goal of sclerotherapy is to induce damage to the endothelial wall resulting in permanent fibrous occlusion of the vessel, she said, explaining that too little damage – from either low concentration or low volume of sclerosant – will result in thrombosis of the vessel, which will recanalize and be ineffective, whereas too much damage – from either high concentration or high volume of sclerosant – will cause extravasation and side effects such as necrosis and pigmentation.
Detergent sclerosants are the ideal sclerosants in most cases, with a few exceptions: For matting or fine telangiectasias, glycerin is often more effective, Dr. Mann said.
For patients with severe allergies, she recommended using hypertonic saline, as there have been documented cases of allergic reaction to both sodium tetradecyl sulfate and polidocanol.
Also, use compression (20-30 mm Hg) following sclerotherapy in all patients to minimize complications, she said.
This reduces the thrombophlebitic reaction and risk of deep vein thrombosis, increases the direct apposition of the treated vein wall, and thus enhances the effectiveness of the sclerosant while decreasing the incidence of recanalization and hyperpigmentation.
Patients' expectations can be managed by reminding them that multiple treatments are usually required, that final results may not be seen for weeks or months, and that treatment induces improvement – not perfection – and doesn't eliminate a genetic tendency to form more troublesome leg veins, she said.
Dr. Mann disclosed that she is a consultant for Bioform/Mertz Aesthetics. She discussed off-label and non–FDA approved sclerosants. SDEF and this news organization are owned by Elsevier.