
Key points
- Approximately 15% to 20% of office gynecologic visits are for the evaluation of abnormal uterine bleeding (AUB), and 25% to 50% of gynecologic surgeries are performed to address menstrual dysfunction.
- Office hysteroscopy and saline infusion sonography are essential skills for the practicing gynecologist. Learn them and use them liberally.
- Inherited and acquired disorders of coagulation, as well as liver and renal diseases, frequently present with symptoms of abnormal uterine bleeding.
- Liberal use of endometrial biopsy is encouraged in women over 35 years of age at risk for endometrial hyperplasia and cancer.
- About 20% to 30% of teens with irregular heavy menses have a major bleeding diathesis.
- Medical therapy is the standard unless uterine pathology is present.
Half of all hysterectomies in the United States are performed to treat abnormal uterine bleeding. Of these, approximately 20% are performed in women with a normal uterine size.1 However, when the uterus appears normal, without adenomyosis or uterine pathology, it is imperative that the clinician perform a thorough evaluation before resorting to hysterectomy.
Abnormal uterine bleeding is defined as excessive, erratic, or irregular bleeding in the presence or absence of intracavitary or uterine pathology. It may be associated with structural or systemic abnormalities. In contrast, dysfunctional uterine bleeding (DUB) is associated with anovulatory menstrual cycles. It is not caused by pelvic pathology, medications, systemic disease, or pregnancy.
Abnormal bleeding is associated with an array of symptoms. Frequent complaints include heavy or prolonged menstrual flow, social embarrassment, diminished quality of life, sexual compromise, and the need to alter lifestyle. Pain is not a common presenting symptom unless it is associated with the passage of large blood clots.
The following menstrual patterns are associated with DUB:
- Oligomenorrhea. A cycle length of more than 35 days
- Polymenorrhea. A cycle length of less than 21 days
- Amenorrhea. The absence of menses for 6 months or 3 consecutive cycles
- Menorrhagia. Heavy or increased flow occurring at regular intervals, or a loss of more than 80 mL of blood
- Metrorrhagia. Irregular episodes of bleeding
- Menometrorrhagia. A longer duration of flow occurring at unpredictable intervals
- Postmenopausal bleeding. Bleeding that occurs more than 12 months after the last menstrual cycle
Basic evaluation and management of abnormal uterine bleeding
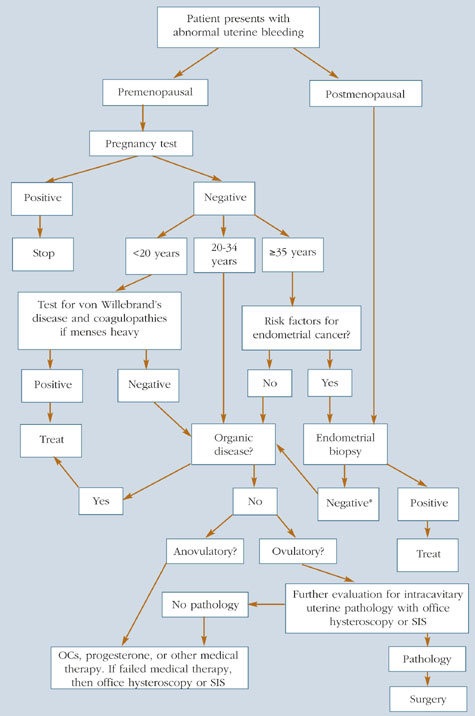
*If still bleeds, then SIS or hysteroscopy
SIS=saline infusion sonography
Prevalence and pathophysiology
Although we lack precise figures regarding the prevalence of abnormal uterine bleeding, it is estimated that 9% to 30% of reproductive-age women have menstrual irregularities requiring medical evaluation.2 Approximately 15% to 20% of office gynecologic visits are scheduled for the evaluation of abnormal uterine bleeding, which is exceeded only by vaginitis as a chief complaint. In addition, 25% to 50% of gynecologic surgical procedures are performed to address menstrual dysfunction.
Normal menstruation is triggered by fluctuations in the hypothalamic-pituitary-ovarian axis that lead to denudation and sloughing of the endometrium. This hemorrhage is followed by prompt hemostasis and repair. Low physiologic levels of estrogen prime the endometrium, while the normal secretion of progesterone from the corpus luteum stabilizes it, decreasing vascular fragility and supporting the endometrial stroma. Platelets and fibrin are necessary for endometrial hemostasis. Deficiencies in either factor may result in heavier menstruation.
DUB occurs when there is inadequate progesterone secretion to stabilize the endometrium. Anovulatory bleeding can be episodic or continuous. Patients with anovulatory cycles typically do not experience premenstrual tension, breast discomfort, increased mucoid vaginal discharge, or cramping and bloating, all characteristic of ovulatory cycles. Although ovulatory cycles are predictable, erratic bleeding may occur when they coexist with intracavitary lesions, including polyps and fibroids.
Anovulatory cycles typically are associated with puberty and the perimenopausal years. In puberty, the immature hypothalamic-pituitary-ovarian axis has not yet developed the necessary hormonal feedback to sustain the endometrium. In perimenopause, the decline of inhibin and rise in follicle-stimulating hormone (FSH) levels reflect the loss of follicular activity and competence.
In some cases, severe anemia can cause incessant menstrual blood loss. Typical complaints of anemia include fatigue, unusual food cravings (pica), and headaches. Severe anemia also can cause fainting, exercise-induced fatigue, shortness of breath, congestive heart failure, and/or the inability to perform routine activities. Unless it is a chronic condition, DUB is rarely associated with the need for a blood transfusion. Hemorrhagic shock and death are rare sequelae.
Diagnosis
Diagnosis involves 3 main components:
- A detailed medical history and review of systems. This should alert the physician to the possible etiology of a patient’s menstrual dysfunction (Table 1). Inherited and acquired disorders of coagulation, as well as liver and renal diseases, frequently present with symptoms of abnormal uterine bleeding.
- A physical examination. The exam must be comprehensive, even in the presence of heavy bleeding, focusing on the vagina, cervix, uterus, and adnexa to exclude pathology.
- Appropriate laboratory studies based on the focused clinical history and any physical findings. Pregnancy testing is necessary in all sexually active premenopausal women. In addition, women with profuse menorrhagia and a normal uterine size should be screened for von Willebrand’s disease, since 13% to 20% of women offered surgical intervention have the subtle form of Type I disease. (In women, von Willebrand’s disease most commonly presents as DUB.) Obviously, medical therapy is paramount for women with von Willebrand’s disease; hysterectomy or other surgical treatment should not be the first option.