Serotonin. Reduced 5-HT transporter binding has been shown in obese women with BED.15 Their 5-HT binding improved and binge eating subsided with group psychotherapy and fluoxetine, although the women continued to gain weight.
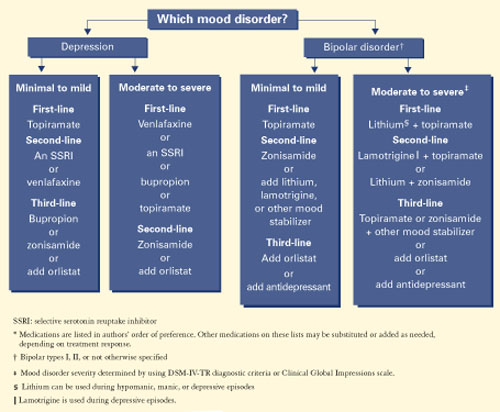
Figure 2 Medication options for BED with obesity and a mood disorder*
Dopamine. Obese patients who compulsively overeat may have lower levels of dopamine D2 receptors than do normal-weight controls.16
Genetic factors. In severely obese patients (body mass index 44±2), those with a DSM-IV diagnosis of BED exhibited mutations of the melanocortin 4 receptor gene, which affects the anorectic properties of alpha melanocyte-stimulating hormone.17
Familial factors associated with BED include parental depression and obesity.18
Psychosocial correlates include physical and sexual abuse, bullying by peers, and discrimination because of being overweight.19
Treatment recommendations
Few systematic studies have examined BED treatment. Emerging research suggests that behavioral weight-loss treatment, specialized psychotherapies, and medications may be effective in some patients with BED.4,6,8
Behavioral weight-loss treatment’s main goal is to manage the patient’s weight with a lower-calorie, healthy diet and to increase exercise.20,21
Over the short term (<1 year), behavioral weight-loss treatment produces similar weight loss in obese patients with or without BED; long-term results in both groups, however, have not been satisfactory.20,21 No studies have examined the efficacy of specialized diets (such as low-carbohydrate regimens) in patients with BED.
Specialized psychotherapy’s goal is to modify bingeeating behavior with behavioral self-management strategies, reducing interpersonal dysfunction and stress, and/or managing affective dysregulation.
Cognitive-behavioral therapy (CBT) and interpersonal therapy (IPT) have been effective in reducing binge eating, both acutely and for up to 12 months4,20-24 but less effective in achieving and maintaining weight loss. Patients who achieve remission in binge eating after undergoing CBT or IPI often experience modest but stable weight loss.20-22 For example, in a comparison study of CBT and IPT:
- After 20 weekly sessions, patients whose binge eating was in remission lost weight (mean body mass index [BMI] −0.5 ± 1.5 kg/m2), whereas those who continued to binge gained weight (mean BMI +0.4 ±2.0 kg/m2).
- At 12 months’ follow-up, patients still in remission continued to lose weight (mean BMI −1.0 ± 3.0 kg/m2), whereas those no longer in remission gained weight (mean BMI +0.7 ±2.9 kg/m2[P = 0.01]).22
Self-help and dialectical behavioral therapy (DBT) may also help reduce binge eating in BED. As with CBT and IPT, they are less effective in weight loss. In the only controlled study of DBT,24 patients achieved an average 2.5-lb weight loss after 20 weeks of DBT, compared with an average 0.6-lb weight gain in the control group. This difference was not significant, and the report did not include data on weight loss maintenance.
In summary, CBT may be more effective than behavioral weight loss treatment for reducing binge eating, but behavioral weight loss is more effective for weight loss.
Medications for BED
Medications that have been tried for BED include antidepressants, appetite suppressants, and anticonvulsants.25,26 Antidepressants are used to treat BED because:
- BED is often associated with depressive symptoms and disorders.
- BED is related to bulimia nervosa, and placebo-controlled trials have shown that the binge eating of bulimia nervosa responds to several classes of antidepressants. The selective serotonin reuptake inhibitor (SSRI) fluoxetine is the only medication indicated for treating any eating disorder (bulimia nervosa).
- Bupropion and venlafaxine—a serotonin-norepinephrine reuptake inhibitor (SNRI)—have weight-loss properties.
SSRIs are the most extensively studied antidepressants for treating BED. SSRIs have weightloss properties, but only short term.25-26 Citalopram, fluoxetine, fluvoxamine, and sertraline have reduced binge eating and body weight more effectively than placebo during 6 to 9 weeks of treatment (Table 2).25-26 However, one controlled study23 showed that fluoxetine was not significantly more effective than placebo in reducing binge frequency or body weight after 16 weeks.
TCAs. Studies of tricyclic antidepressants (TCAs) for BED are sparse, and results have been mixed. In one trial, imipramine was similar to placebo in reducing binge frequency and body weight. In a placebo-controlled study of patients with nonpurging bulimia nervosa, desipramine reduced binge eating but had no effect on body weight.25,26
Table 2
Drug therapies shown to be effective for BED*
| Medication | Binge eating | Weight | Depression | Study size | Duration (weeks) | Dosage (mg/d) |
|---|---|---|---|---|---|---|
| Antidepressants | ||||||
| Citalopram | + | + | − | 38 | 6 | 20 to 60 |
| Fluoxetine † | + | + | + | 60 | 6 | 20 to 80 |
| Fluvoxamine | + | + | − | 85 | 9 | 50 to 300 |
| Sertraline | + | + | − | 34 | 6 | 50 to 200 |
| Appetite suppressant | ||||||
| Sibutramine | + | + | + | 60 | 12 | 15 |
| Anticonvulsant | ||||||
| Topiramate | + | + | − | 61 | 14 | 50 to 600 |
| + Improvement | ||||||
| − No improvement | ||||||
| * Randomized, controlled trials. Antidepressants were studied in patients with BED; sibutramine and topiramate were studied in patients with BED and associated obesity. | ||||||
| † One 16-week trial of fluoxetine for BED (reference 23) did not show statistically significant differences in post-treatment binge frequency or body-mass index. | ||||||
Venlafaxine. In a retrospective review of 35 consecutive obese women with BED, venlafaxine, mean 222 mg/d for 28 to 300 days (median 120 days), reduced binge eating, body weight, and depressive symptoms.27