Clinical snapshot of BED
Managing patients with binge-eating disorder (BED) often requires behavioral, medical, and psychiatric interventions.
These patients suffer from recurrent episodes of distressing, uncontrollable overeating, but they do not purge or show other compensatory weight-loss behaviors common to bulimia nervosa1 and anorexia nervosa.2-10 As a result, they are often overweight or obese and may have obesity-related illnesses, such as hypertension or type 2 diabetes. Mild to severe depression—unipolar or bipolar—is a common psychopathology.
Because no one treatment fits all patients with binge eating disorder, their management usually requires an individualized program of:
- behavioral weight control
- psychotherapy
- and sometimes medications.
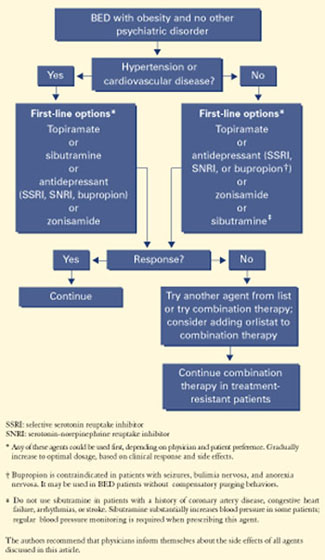
In our weight management clinic, we consider medication options based on patient preference and whether BED is uncomplicated (Figure 1) or coexists with a mood disorder (Figure 2).
This article presents the evidence on which we base our comprehensive approach. General psychiatrists with knowledge of BED can treat patients with this eating disorder, although complicated cases may require referral for specialized treatment.
Figure 1 Medication options for uncomplicated BED
Clinical characteristics
Psychiatric comorbidity. BED often occurs in patients with mood, anxiety, substance-abuse, impulsecontrol, and personality disorders.4,6,10-12 Mood disorder—particularly depression—appears to be the most common comorbidity. BED can occur with bipolar disorder12—a comorbidity that in our experience is underrecognized both clinically and in the literature.
Patients with BED and bipolar disorder show increased impulsivity and mood lability. As bipolar II disorder and other “soft-spectrum” forms are more common than bipolar I disorder, BED is also more likely to occur with hypomania than mania.
Overweight. Not surprisingly, BED is associated with overweight and obesity.5,8,9,11 Not all patients with BED are overweight or obese, but most who participate in clinical trials of BED treatments are at least overweight. BED has been reported in up to:
- 30% of participants in weight-loss programs7
- 70% of participants in groups such as Overeaters Anonymous
- 50% of patients who seek bariatric surgery.5
In our experience, patients are often more distressed by their weight than by their binge eating, depression, or anxiety. Indeed, overweight and obesity are the usual reasons patients with BED present for treatment at our center.
Diagnosis. BED’s validity as a clinical diagnosis has been controversial since the disorder was first included in DSM-IV (Table 1).3 Debate continues about some definitions in the DSM criteria, including what amount of food is “definitely larger” than most people would eat and what is “loss of control over eating.”
Nevertheless, screening for BED is relatively easy. Clinicians may use the eating disorder section of the Structured Clinical Interview for DSM-IV or the Eating Disorders Examination. Alternatively, simply ask patients if they have episodes of uncontrollable overeating, during which they eat unusually large amounts of food and their eating feels out of control.
Course. BED begins in adolescence or adulthood. Disease course is variable, with periods of remission, recurrence, and chronicity.6,7,10 Interestingly, one prospective study showed that even if the binge eating resolves, persons may still develop obesity.13
Prevalence. BED affects 1.5% to 3% of the U.S. population. It is more common in women than men, equally prevalent in whites and blacks, and more prevalent than anorexia nervosa and bulimia nervosa combined.11,14 Subthreshold BED—such as obesity with infrequent or nondistressing binge eating—appears to be much more common,10 although no data are available.
Theories of binge eating
BED’s cause is unknown, but biological, familial, and psychosocial factors have been implicated.
Biological factors. The neurotransmitters serotonin (5-HT) and dopamine—as well as various peptides—have been shown to help regulate feeding behavior.10
Table 1
Diagnostic criteria for binge-eating disorder*
|
| * Research criteria, DSM-IV-TR appendix B. |
| Source: Reprinted with permission from the Diagnostic and statistical manual of mental disorders, 4th edition, text revision. Copyright 2000. American Psychiatric Association. |