Dr. Nguyen is from the Creighton University School of Medicine, Phoenix Regional Campus, Arizona. Drs. Glembocki and Patel are from Southwest Skin Specialists, Phoenix.
The authors report no conflict of interest.
Correspondence: Austin Huy Nguyen, MD, MS, Creighton University School of Medicine, Phoenix Regional Campus, 350 W Thomas Rd, Phoenix, AZ 85015 (AustinNguyen@creighton.edu).
Multinucleate cell angiohistiocytoma (MCAH) is a rare cutaneous entity described as grouped erythematous to violaceous papules. Histopathologic findings include vascular proliferations with multinucleate giant cells and dermal fibrosis. We report a case of MCAH in an 83-year-old white man affecting both the right anterior thigh and left posterior calf. Additionally, the pathogenesis of MCAH and different therapeutic modalities are reviewed.
Multinucleate cell angiohistiocytoma (MCAH) is a rare underrecognized cutaneous tumor presenting as erythematous to violaceous papules.
Although it clinically mimics Kaposi sarcoma, MCAH may be distinguished histopathologically by negative immunostaining for human herpesvirus 8.
Surgical excision and laser therapies are definitive treatments for MCAH, which is a benign lesion.
References
Multinucleate cell angiohistiocytoma (MCAH) is a rare benign, soft-tissue tumor first described in 1985 by Smith and Jones1 that presents clinically as erythematous to violaceous papules most commonly affecting females on the dorsal aspect of the hands and face.2 Multinucleate cell angiohistiocytoma is histologically characterized by vascular and histiocytic proliferations with dermal fibrosis. Few cases have been reported of lesions affecting the lower extremities. We report a case of MCAH affecting the legs.
Case Report
An 83-year-old white man with a history of basal cell carcinoma presented for evaluation of grouped, well-circumscribed, soft, red-violet, painless papules on the right anterior thigh that had been present for 8 months (Figure 1A). A review of symptoms was negative for immunologic, respiratory, and hematologic changes. The patient’s medical history also was remarkable for prostate cancer treated with radiation 18 years prior as well as right hip and left knee implants. The initial clinical impression was Kaposi sarcoma or a granulomatous disorder.
Histopathologic evaluation of a deep shave biopsy initially determined the lesion to be scar tissue without other pathologic findings. The patient returned to the clinic 12 months later for a complete skin examination given his history of skin cancer. Compared to clinical photographs taken a year prior, new violaceous papules were noted on the right thigh (Figure 1B) and left calf. Furthermore, there was no recurrence of the lesion at the prior biopsy site. Shave biopsies of the papules on the right thigh and left calf demonstrated similar histologic findings to each other. There was a mild increase in the number of small blood vessels in the superficial dermis (Figure 2A). A mild perivascular lymphocytic infiltrate surrounded some of these blood vessels. The endothelial cells had small nuclei with no evidence of nuclear pleomorphism. Careful examination of the interstitial dermis revealed scattered multinucleate cells with angulated cytoplasm (Figure 2B). Immunostaining for CD31 and human herpesvirus 8 were negative, excluding an infiltrative vascular tumor and Kaposi sarcoma, respectively. The diagnosis of MCAH was made based on the histopathologic findings.
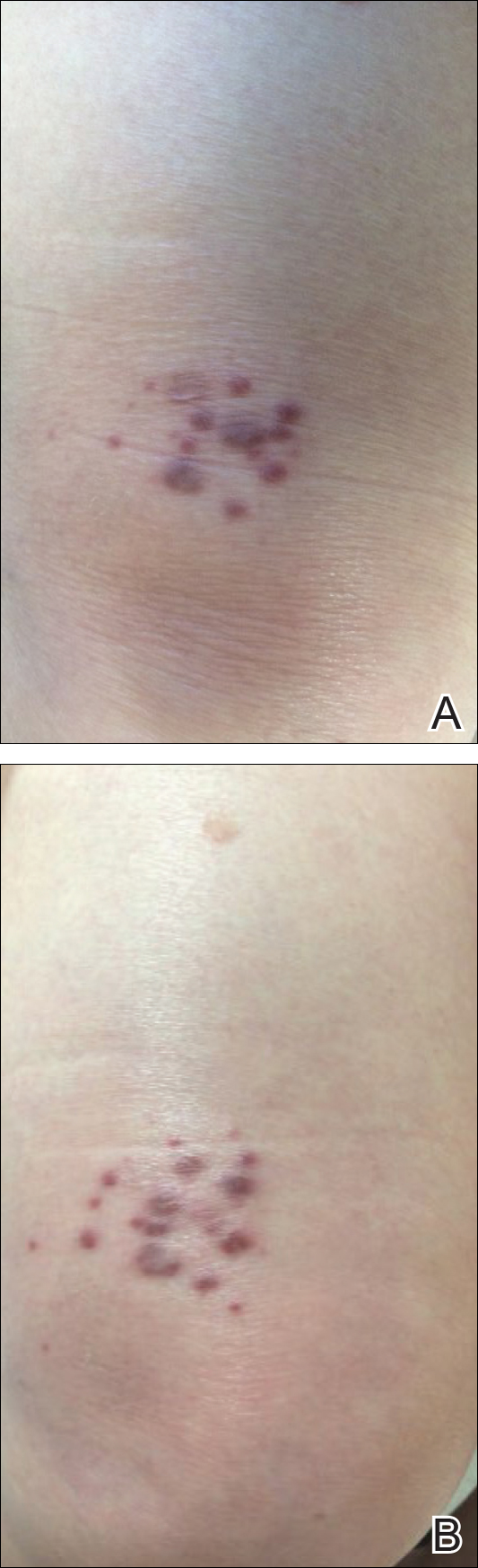
Figure 1. Multinucleate cell angiohistiocytoma at initial visit presenting as grouped, well-circumscribed, soft, red-violet, painless papules on the right anterior thigh (A), with new lesions noted on the right thigh at 1-year follow-up.
Figure 2. Histologic evaluation of multinucleate cell angiohistiocytoma demonstrated an increased number of small blood vessels in the superficial dermis (A) and large angulated multinucleate cells (B)(both H&E, original magnifications ×40 and ×100).
At 1-year follow-up, the condition was stable with no gross changes in the lesions based on prior photographs. Once again, there was no recurrence of the excised lesions at both biopsy sites.