Medications typically intended for short-term use during acute illness are sometimes continued after discharge without documented indication [51]. Poudel et al found that in 206 patients 70 years of age and older discharged to residential aged care facilities from acute care, at least 1 PIM was identified in 112 (54.4%) patients on admission and 102 (49.5%) patients on discharge [11]. Commonly prescribed PIM categories, at both admission and discharge, were central nervous system, cardiovascular, gastrointestinal, and respiratory drugs and analgesics [6,11,52,53]. Of all medications prescribed at admission (1728), 10.8% were PIMs, and at discharge, of 1759 medications, 9.6% were PIMs. Of the total 187 PIMs on admission, 56 (30%) were stopped, and 131 (70%) were continued; 32 new PIMs were introduced [11].
Morandi et al in 2011 conducted a prospective cohort study including 120 patients age ≥ 60 who were discharged after receiving care in a medical, surgical, or cardiovascular ICU for shock or respiratory failure. The percentage of patients prescribed at least 1 PIM increased from 66% at pre-admission to 85% at discharge. The number of patients with 0 PIMs dropped from 34% at preadmission to 14% at discharge, and the number of patients with 3 or more PIMS increased from 16% at preadmission to 37% at discharge. While it is possible that these drugs may be appropriate when started during an acute illness in the ICU (eg, stress ulcer prophylaxis with H2-antagonists in mechanically ventilated patients), most should have been discontinued at ICU and/or hospital discharge [21].
Inappropriate prescriptions of proton pump inhibitors (PPIs) in hospital and primary care have been widely reported [54,55]. In a study conducted by Ahrens et al in 31 primary care practices, for 58% (263/506) of patients discharged from 35 hospitals with a PPI recommendation in hospital discharge letters, an appropriate indication was missing. In 57% of these cases general practitioners followed this recommendation and continued the prescription for more than 1 month [54]. The strongest factor associated with appropriate and inappropriate continuation of PPI after discharge was PPI prescription prior to hospitalization [54]. Although PPIs are safe, they can cause adverse effects. PPI intake has been found to have a significant association with risk of community-acquired pneumonia [56,57], hip fractures [58], Clostridium difficile-associated diarrhea [55,61,62], and to reduce the therapeutic effects of bisphosphonates [59] and low-dose aspirin [60].
Unintentional medication continuation is not a problem isolated to a single drug class or disease [63]. Scales et al evaluated rates of and risk factors for potentially unintentional medication continuation following hospitalization in a population of elderly patients (≥ 66 years) [51]. They created distinct cohorts by identifying seniors not previously receiving four classes of medications typically used to treat or prevent complications of acute illness: antipsychotic medications; gastric acid suppressants (ie, histamine-2 blockers and proton pump inhibitors); benzodiazepines; and inhaled bronchodilators and steroids [51]. Prescription without documented indication occurred across all medication classes, from 12,209 patients (1.4 %) for antipsychotic medications to 34,140 patients (6.1 %) for gastric acid suppressants [51].
Several potential risk factors were considered. The relationship between multimorbidity and polypharmacy is well described in the literature, and several studies have identified a positive association between the number of drugs and the use of PIMs [64–66]. Conversely, Poudel et al did not find any association between polypharmacy and PIM use [11]. Associations were found between the use of PIMs, frailty status, and cognitive decline of patients at admission and at discharge [11], while no association was observed with age, gender, in-hospital falls, delirium, and functional decline [11,67]. Other potential risk factors of a high number of PIMs at discharge were a high number of pre-admission PIMs, discharge to a location other than home, and discharge from a surgical service [1,6,68,69]. Length of ICU stay and mechanical ventilation had a positive influence on the number of PIMs used by acutely ill older patients [11,63,69]. In the study of Scales et al, the greatest absolute risk factor across all medication groups was longer hospitalization. The increased OR for medication continuation after a hospitalization lasting more than 7 days ranged from 2.03 (95% CI 1.94–2.11) for respiratory inhalers to 6.35 (95% CI 5.91–6.82) for antipsychotic medications [51].
Inappropriate Medications: Where and How to Intervene?
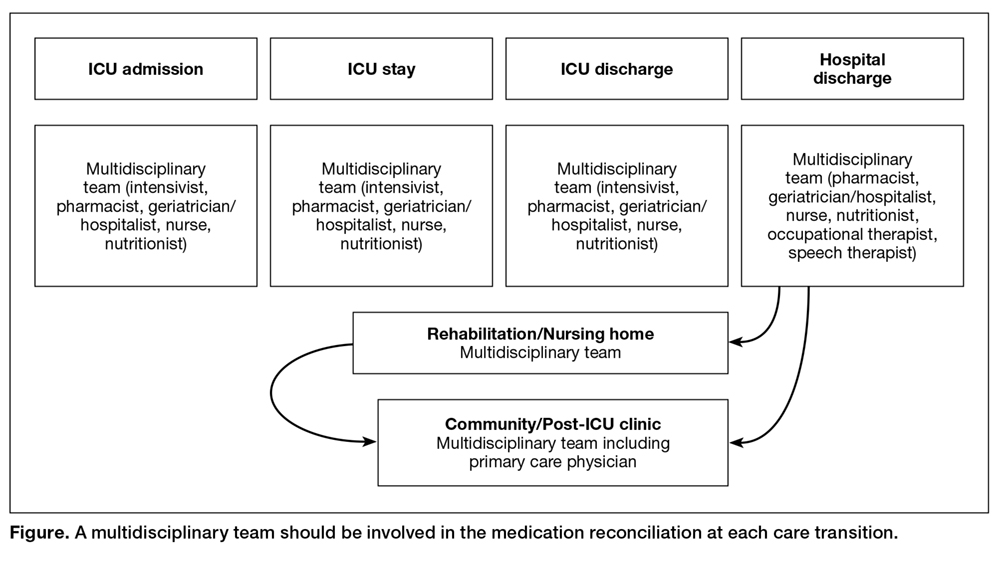
Early detection of PIMs may prevent adverse drug events and improve geriatric care in older adults [13,70]. PIM prevalence can often be a useful indicator of prescribing quality [2]. Appropriate interventions and an improved quality of prescribed medications require appropriate assessment tools to decrease the number of patients discharged on these medications [71,72]. Medication reconciliation is the process of avoiding inadvertent inconsistencies within a patient’s drug regimen, which can occur during transitions in different setting of care [73]. A multidisciplinary team should be involved in the medication reconciliation at each care transition to reevaluate medications use according to the clinical conditions, cognitive/functional status and the coexistence of geriatric syndromes (eg, dementia, malnutrition, delirium, urinary incontinence, frailty) (Figure).
Medication reconciliation should be performed at ICU admission, ICU discharge, and hospital discharge. At discharge, effective communication between the hospital team and the outpatient provider should include timely, accurate, and complete documentation of indication, dosage, frequency, route of administration, and planned duration of use of all medications. This approach would allow the primary care practitioners and the caregivers to understand the reason why the patient is on a given medication, and thus providing them with the necessary information to discontinue or continue the therapy. Patients might then be discharged home or to rehabilitation or nursing home settings. A post discharge follow-up should then be performed in each setting to reevaluate the appropriateness of medications prescribed in the previous settings or to evaluate the necessity to initiate necessary drugs according to the patients’ conditions.