Criteria for the Evaluation of Inappropriate Medications Prescription
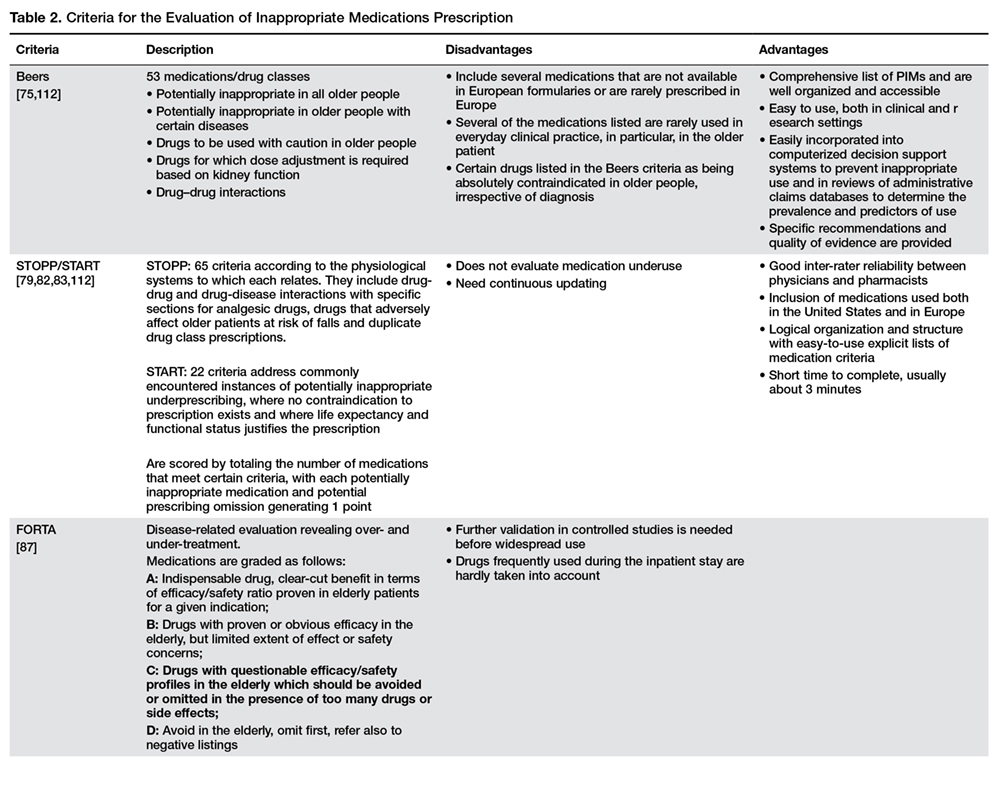
Explicit criteria derived from expert reports or published reviews are available (Table 2).
These have high reliability and reproducibility but focus mainly on specific drugs and disease states. Although these criteria address some aspects of prescribing in older patients, they seldom consider the frailty of such patients. The omission of health status from established prescribing tools may help explain the lack of clinical benefit from algorithm-based medication reviews [74]. The American Geriatrics Society (AGS) Beers criteria for potentially inappropriate medications use in older adults is an explicit list of PIMs best avoided in older adults in general and in those with certain diseases or syndromes, prescribed at reduced dosage, with caution or carefully monitored [75]. The Beers criteria are commonly used, and they do measure some surrogates of frailty.
They were originally developed in 1991 [76] for use in the older nursing home population and have been subsequently updated to apply to all persons older than 65 years, regardless of their place of residence [18]. The recently updated Beers criteria divides medications into 3 main categories according to major therapeutic classes and organ systems: 34 medications are considered potentially inappropriate, independent of diagnosis; 14 are to be avoided in older adults with certain diseases and syndromes that can be exacerbated by the listed drug, and 14 others are to be used with caution in older adults [18]. In 2015 two major components were added: (1) drugs for which dose adjustment is required based on kidney function and (2) drug-drug interactions [18,77].
Beers criteria PIMs have been found to be associated with poor health outcomes, including confusion, falls, and mortality [7,75,78]. The STOPP (Screening Tool of Older Person’s potentially inappropriate Prescriptions) and START (Screening Tool to Alert doctors to the Right Treatment) are evidence-based sets of criteria that were developed in Ireland and updated in October 2014, including some of the new criteria for direct oral anticoagulants, drugs affecting or affected by renal system and anti-muscarinic/anticholinergic agents [79].
The updated STOPP/START criteria are considered more sensitive and specific for the detection of inappropriate prescription than the previous version [80,81]. The criteria are organized according to the physiological systems to which each relates, thereby enhancing their usability and refer to classes of medications [80,81]. The STOPP and START tools are scored by the summary of the number of medications that meet certain criteria, with each potentially inappropriate medication and potential prescribing omission generating 1 point [82]. Previous research indicates that a 0.5–decrease in STOPP score yielded a 17% risk reduction in medication-related hospital admissions [83]. Some studies that compared STOPP and Beers criteria revealed a greater correlation between drug-related adverse events and PIMS defined with the former, suggesting that the STOPP criteria may be more helpful clinically [84,85].
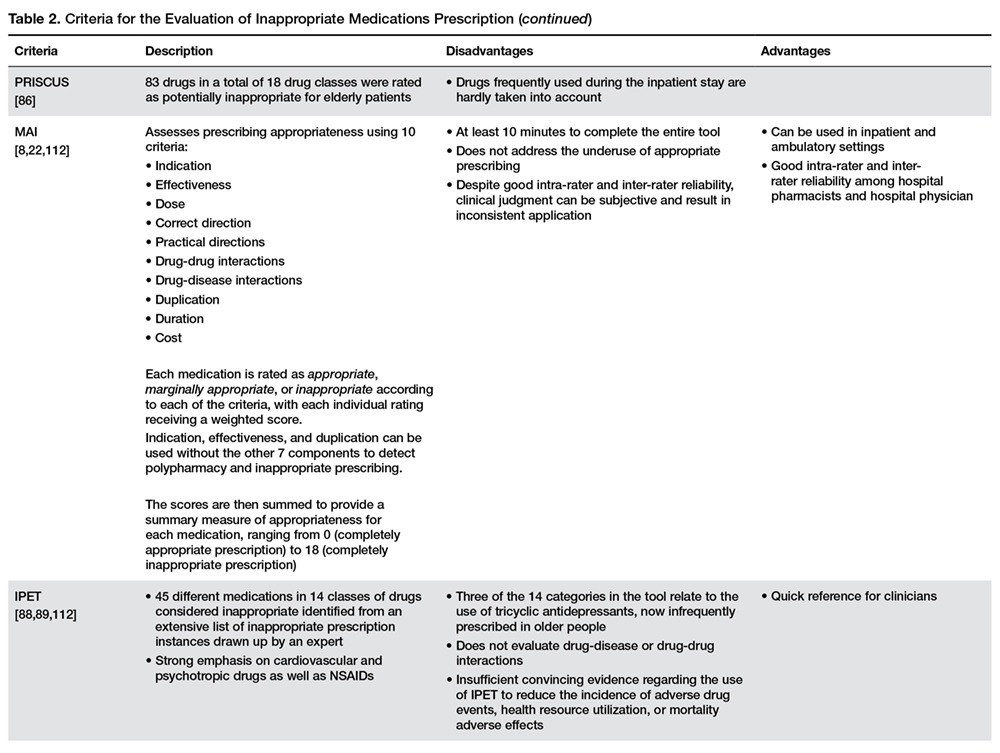
Several other sets of criteria have been published to identify PIMs, such as the FORTA (Fit for the Aged) and the PRISCUS [86] criteria. FORTA allows a disease-related evaluation revealing over-treatment and under-treatment, and medications are graded as follows: A, indispensable drug, clear-cut benefit in terms of efficacy/safety ratio proven in elderly patients for a given indication; B, drugs with proven or obvious efficacy in the elderly, but limited extent of effect or safety concerns; C, drugs with questionable efficacy/safety profiles in the elderly which should be avoided or omitted in the presence of too many drugs or side effects; D, avoid in the elderly, omit first, refer also to negative listings. Negative lists such as PRISCUS, which provide an explicit listing of drugs, independent of the diagnosis, are easy to use. On the other hand, constant updates are needed, and such lists carry the risk of an assumption that drugs not listed would be appropriate in every case [87]. Both sets of criteria have in common that they refer to long-term medication and drugs frequently used during the inpatient stay, such as antibiotics, are hardly taken into account [87].
The Medication Appropriateness Index measures overall prescribing quality through 10 separate but interrelated domains [8]. Three components are used to detect PIMs: indication, effectiveness, and duplication. However, it does not give any precise guidance in relation to specific medicines and therefore has limited application for objectively defining PIMs.
Another prescribing quality assessment tool is the Inappropriate Prescribing in the Elderly Tool (IPET), which consists of a list of the 14 most prevalent prescription errors identified from an extensive list of inappropriate prescription instances drawn up by an expert Canadian Consensus Panel [88,89].
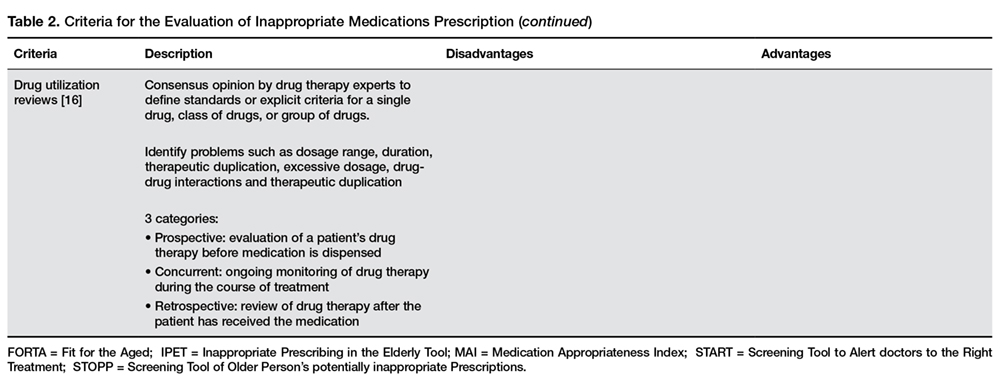
Another approach to assess the appropriateness of drugs prescribed for older people is the use of Drug Utilization Reviews (DURs) [16]. DURs use consensus opinion by drug therapy experts to define standards or explicit criteria for a single drug, class of drugs, or group of drugs [16]. DURs typically use retrospective information from large, nonclinical administrative databases to identify problems such as dosage range, duration, therapeutic duplication, and drug interactions [90, 91]. Monane et al [92] evaluated a program designed to decrease the use of PIMs among the elderly through a computerized online DUR database. Computer alerts triggered telephone calls to physicians by pharmacists to discuss a potential problem and any therapeutic substitution options. From a total of 43,007 telepharmacy calls generated by the alerts, they were able to reach 19,368 physicians regarding 24,266 alerts (56%). The rate of change to a more appropriate therapeutic agent was 24% (5860), but ranged from 40% for long half-life benzodiazepines to 2% to 7% for drugs that theoretically were contraindicated by patients’ self-reported history [92].