Computerized Support Systems to Reduce Inappropriate Prescribing in the Elderly
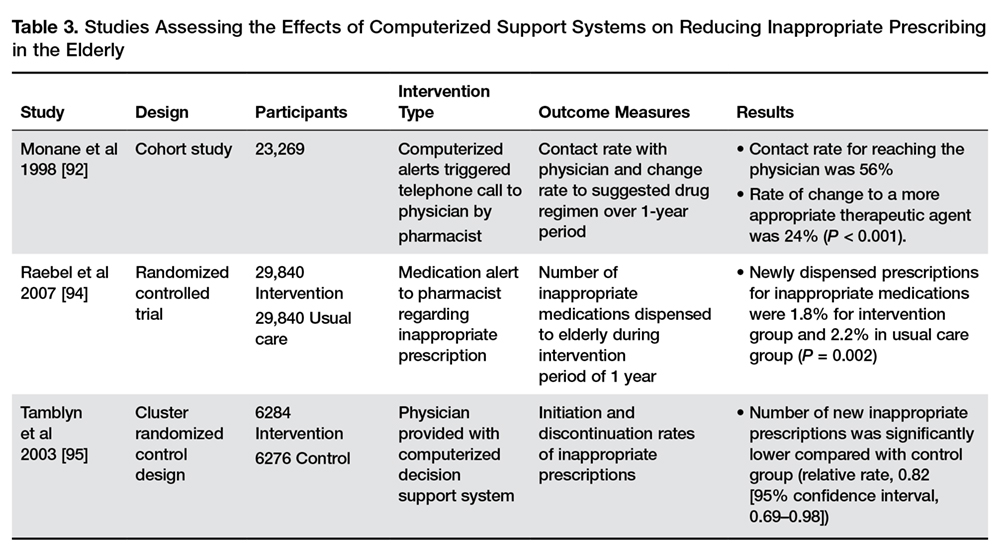
Other potential solutions for reducing inappropriate medications may include continuing medical education, electronic medical records surveillance, routine clinical evaluation, and/or improved hand-off communication between discharging and accepting providers. Incorporating this assessment of medication appropriateness into the medication reconciliation process when patients are discharged or transferred out of the ICU has the potential to enhance patient safety [21,93]. A randomized controlled trial conducted by Raebel et al [94] reported the effectiveness of a computerized pharmacy alert system plus collaboration between health care professionals for decreasing potentially inappropriate medication dispensing in elderly patients. Another study showed that computer-based access to complete drug profiles and alerts about potential prescribing problems reduced the occurrence of potentially inappropriate prescriptions [95]. A summary of these studies is shown in Table 3.
Interdisciplinary Teams to Reduce Inappropriate Prescribing in the Elderly
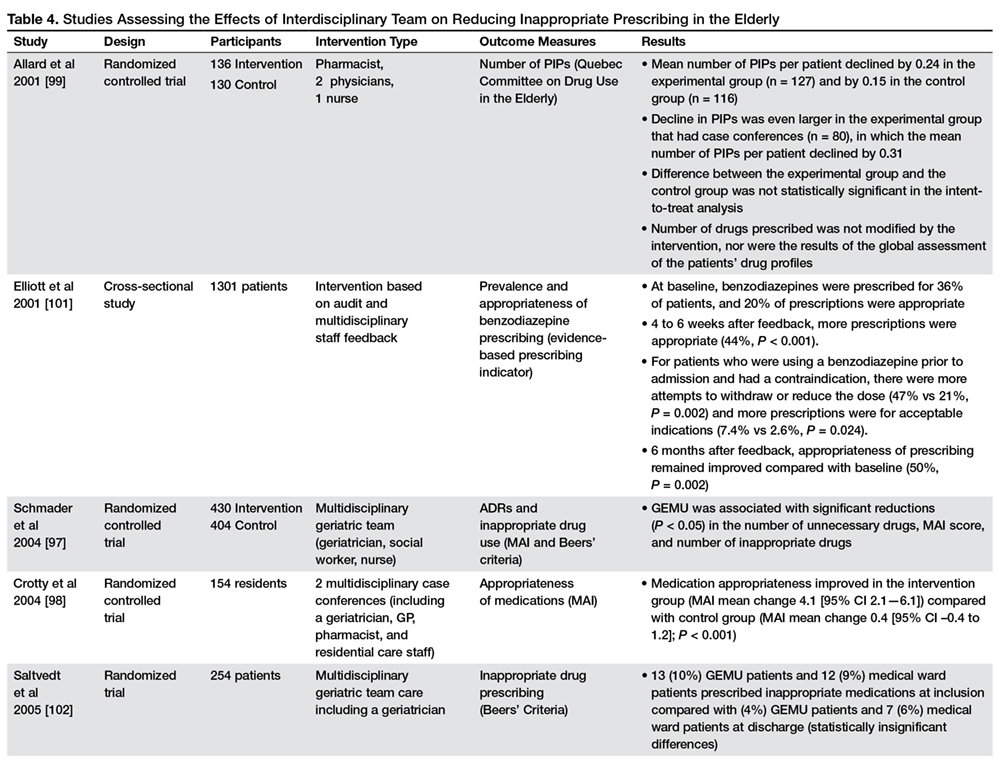
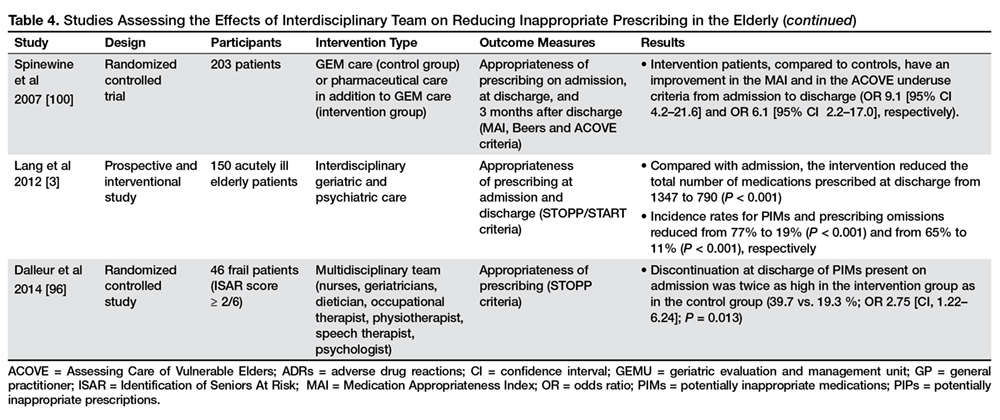
Some studies evaluated the effect of multidisciplinary teamwork in improving inappropriate medication prescribing in the elderly (Table 4).
An interdisciplinary team, involving a geriatrician, together with nurses, dietician, occupational therapist, physiotherapist, speech therapist, psychologist, and psychiatrists, reduced the total number of PIMs prescribed at discharge and serious adverse drug reactions [3,93,96–101]. Conversely, another study showed that patients treated in a geriatrics evaluation and management unit (GEMU) had a statistically significant difference in appropriateness of drug profiles compared with patients in general wards, in terms of prescription of fewer drugs with anticholinergic effects, psychotropic drugs, and cardiovascular drugs [102].
The important role of comprehensive geriatric evaluation to reduce the risk of serious adverse drug reactions and suboptimal prescribing in elderly patients was confirmed by Schmader et al who evaluated the effect of inpatient and outpatient geriatric evaluation and management, as compared with usual care, in reducing adverse drug reactions and suboptimal prescribing in frail elderly patients. Between discharge and 12 months, patients receiving care from geriatric evaluation and management clinics had a 35% reduction in the risk of serious adverse drug reactions compared with usual outpatient care [97].
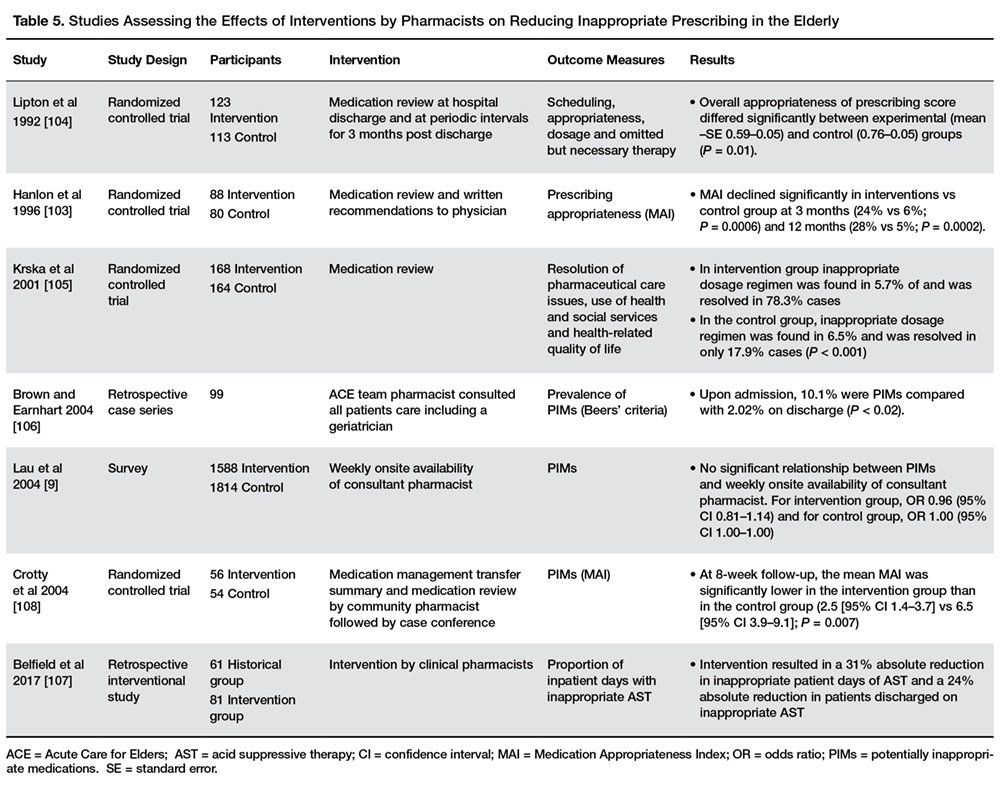
Pharmacists in hospitals can play a significant role in the initiation of changes to patient’s therapy and management [11] (Table 5).
Medication review by the pharmacist in an acute care or primary care setting and at discharge from the ICU and the hospital can reduce inappropriate prescribing and possibly avoid adverse drug effects without adversely affecting health-related quality of life [103–107]. Moreover, a pharmacist transition coordinator was shown to improve aspects of inappropriate use of medicines across health sectors [108]. Different results were showed by Lau et al in a national survey between nursing homes and residents, who found that the presence of a consultant pharmacist had no effect on potentially inappropriate prescriptions [9]. However, they did not specify the extent of the pharmacists’ involvement and it is, therefore, uncertain whether this finding adequately reflects the effectiveness of a consultant pharmacist on the quality of prescribing in nursing homes [93].
Mattison et al recently emphasized that studies of PIMs should determine scenarios in which it is appropriate to prescribe PIMs, moving beyond simply labeling some medications as “potentially inappropriate,” since some PIMs are appropriately prescribed in specific clinical situations [109]. Morandi et al showed that the positive predictive value (PPV) depends on the drug type. Thus, when developing a screening system, one cannot be concerned only with high negative predictive value (NPV), one must consider PPV as well [6]. Screening tools that include medication classes with low PPV will generate false positive “flags” or warnings, which could lead to misguided clinical decisions [6]. The fact that many PIMs are not AIMs also reveals the value of using a multidisciplinary team to identify AIMs from lists of PIMs generated when discharge medication lists are screened [6,110]. Thus, a multidisciplinary team is needed to consider the clinical context to distinguish PIMs from AIMs [6]. Of course, such a team is not available in some settings; when resources are limited, knowledge of which PIMs are most likely AIMs (ie, have high PPVs) could guide the development of computer-based decision support systems or other surveillance approaches that are efficient in that particular setting [6].
Approaches for optimizing prescribing in this population mainly depend on patient needs and comorbidities and most available data are derived from randomized controlled trials involving a single drug. Such trials do not take into account the confounding effects of multiple comorbidities and patient preferences. Therefore, approaches for optimizing prescription management that are available for and validated in younger patients are not applicable to elderly subjects [3,111].