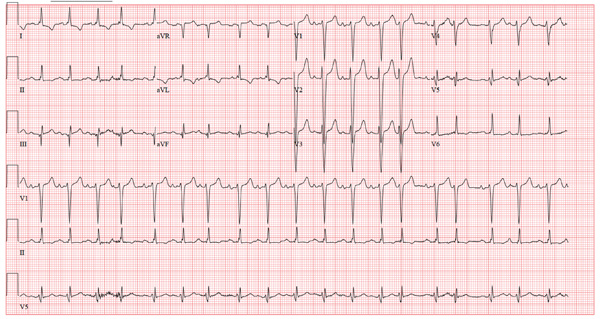
A 38-year-old woman presents to your clinic with a two-year history of palpitations that have not increased in severity or frequency. Although they are bother-some, she has had no chest pain, shortness of breath, dyspnea on exertion, or peripheral edema. She denies any symptoms of tachycardia, bradycardia, syn-cope, or near syncope. She works at a local health club as a Zumba instructor and teaches four spinning classes per week. She recently learned that the health club will be closing. As a result, until she finds another position, she will be without benefits. She states she wants to “get this checked out” before she loses her medical insurance. Medical history is unremarkable, with the exception of a right clavicle fracture sustained at age 15. She began menses at age 12, has never been pregnant, and has never had surgery. Family history is remarkable for hypertension and diabetes. Her parents and three siblings are alive and well. The patient has no known drug allergies. Her medications include ibuprofen as needed for musculoskeletal pain and an oral contraceptive. She denies recreational drug use. The review of systems is unremarkable, and her last menstrual period was 11 days ago. On physical exam, she is a thin, well-developed, athletic-appearing woman in no distress. Her height is 69”, and her weight is 144 lb. Blood pressure is 108/56 mm Hg; pulse, 58 beats/min and regular; respiratory rate, 14 beats/min; and temperature, 98.4°F. There are no murmurs, gallops, or rubs on her cardiac exam. Her lungs are clear. Her abdomen is flat and nontender, with good bowel tones in all quadrants. There is no peripheral edema. Peripheral pulses are full and bounding bilaterally in all four extremities. The neurologic exam is normal. A chemistry panel, complete blood count, lipid panel, and thyroid function studies are ordered; the results are all within normal limits. A transthoracic echocardiogram shows normal valves, normal wall motion, and a left ventricular ejection fraction of 75%. A baseline ECG shows no ectopic beats. She is placed on a continuous rhythm monitor for 10 minutes, and no ectopic, premature, or dropped beats are seen. At that point, the patient remembers that the palpitations often occur just as she starts exercising, then go away once her heart rate is elevated. You have her do jumping jacks in the examination room for 30 seconds, and she states she can feel the palpitations. You quickly obtain an ECG, which reveals the following: a ventricular rate of 117 beats/min; PR interval, 158 ms; QRS duration, 110 ms; QT/QTc interval, 336/468 ms; P axis, 57°; R axis, 15°; and T axis, 153°. What is your interpretation of this ECG?