FIGURE 2
DURATION OF ILLNESS, PAIN, AND PURULENT RHINORRHEA BETWEEN TREATMENT GROUPS
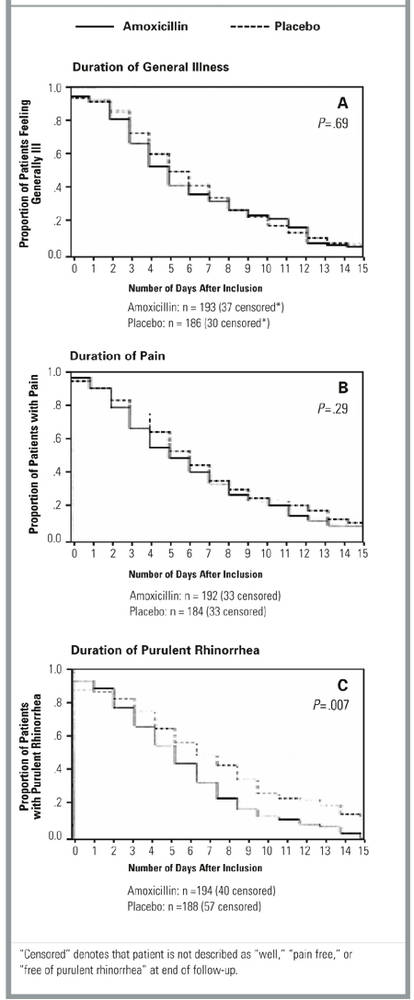
Secondary outcomes
The mean score reduction on the symptom “thick nasal discharge” between day 1 and day 10 is significantly larger in the amoxicillin group than in the placebo group (2.2 vs 1.5, Student’s t test: P <.0001) (Table 3). There is no significant difference in change for any other symptom. Seven patients in the placebo group (3.4%) withdrew before day 10 because of exacerbation of symptoms versus 1 patient (0.5%) in the amoxicillin group (RR 0.25, 95% CI, 0.04-1.56, P = .07). All 8 patients recovered after starting open antibiotic therapy and had no complications or referrals.
The chance of receiving open antibiotic treatment at day 10 follow-up (n = 34: 19 placebo, 15 amoxicillin) or of having to return because of persistent complaints at day 15 (n = 73: 41 placebo, 32 amoxicillin) was not significantly different between the treatment groups (chi-squared test: P = .46 and P = .26, respectively). Diarrhea was more frequent in the amoxicillin group (29% vs. 19%, RR 1.28, CI 1.05-1.57, P = .02). There was no difference in incidence of skin rash, abdominal pain, or vomiting. Absence from work or school was comparable in both treatment groups (RR 0.95, 95% CI, 0.86-1.05, P = .34). Patients in the amoxicillin group took an analgesic an average of 5 times, mainly in the first days of treatment, compared with 4 for the placebo group (Mann-Whitney U test, P = .24).
Other results
The lack of correlation between the estimated and actual treatment demonstrates that masking was maintained. Compliance was good in both groups: 89% of patients in the amoxicillin group and 91% of those in the placebo group took at least 25 of 30 capsules.
Patients from low recruiters were not significantly different from patients enrolled by high recruiters. Included patients had slightly more complaints of pain (58% vs 50%, RR 1.20, CI 1.02-1.42, P = .03) than the 332 eligible but excluded patients registered during the 6-week period. The most frequent reasons for exclusion were the presence of an exclusion criterion (22%), the patient’s refusal to participate (16%), the patient’s request for antibiotic therapy (14%), and lack of time by the FP (10%). Of the 292 patients who agreed to undergo a radiologic examination, about two thirds had abnormalities of the maxillary sinuses.
Discussion
This study produced 3 important findings. First, we found that patients consulting their FP for acute URTI with purulent rhinorrhea do not experience any important benefit from amoxicillin therapy. With treatment, the purulent rhinorrhea disappears more quickly, but this seems to be of little importance in relation to a general recovery. Moreover, amoxicillin therapy increases the risk of diarrhea. We further found that with or without amoxicillin, complaints last long: after 10 days, two thirds of patients still had complaints and about half of the patients still felt ill. The natural course to recovery takes a long time and is not influenced by taking amoxicillin. Finally, we observed that failure to prescribe antibiotics is safe. The placebo group had no complications. A small number of exacerbations occurred, but these responded swiftly to a course of amoxicillin-clavulanate.
To our knowledge, this is the first time that the effect of an antibiotic in adult patients presenting with acute purulent rhinorrhea (but with an otherwise unspecified diagnosis) has been investigated in a randomized, placebo-controlled trial. This trial is in line with a number of other family practice-based pragmatic trials in which patients were included on the basis of respiratory symptoms instead of by diagnosis16,32-37 and in which the emphasis was on practical relevance rather than on diagnostic accuracy.
Since 1995, 6 randomized clinical trials of high methodologic quality11-16 have studied the efficacy of antibiotics in general practice patients suffering from various acute infections of the nasal passages and usually presenting with purulent rhinorrhea. In 3 of these trials, no beneficial effect of antibiotics was found. Study populations consisted, respectively, of patients with a set of clinical symptoms (including purulent rhinorrhea) indicating rhinosinusitis16; patients with clinical suspicion of rhinosinusitis plus sinus abnormalities on conventional radiology11; and patients with clinical suspicion of sinusitis but without the radiologic signs.14 In the 3 other trials, treatment was (more or less) effective. Included were patients with clinical suspicion of sinusitis and abnormalities on CT scan,12 patients with unilateral facial pain and elevated C-reactive protein levels or erythrocyte sedimentation rate,13 and patients with rhinopharyngitis and positive bacteriologic cultures of nasopharyngeal secretions.15 These trials show that antibiotics are efficacious in some patients. In our trial, which probably included a mix of all these populations, we also found more patients in the amoxicillin group to be symptom free after 10 days. Despite a fairly large sample size, however, this difference was too small (less than 15%) to be statistically significant.