Other review articles reach the same conclusion. One article reviewed the literature from 1980 to 1996 and examined 17 prospective clinical trials. Outcomes measured included pulmonary function measures and clinical scores. The researchers recommended that MDI/S be used due to clinical benefit, safety, lower cost, personnel time, and speed and ease of administration.5
A review article from the British literature examined 3 randomized controlled trials involving 51 patients and found no superiority of nebulizer vs MDI/S.6 A similar review article examined 14 randomized controlled trials for beta-agonist delivery for patients aged 5 to 15 with stable asthma. They found no obvious benefit of 1 type of device over another, including nebulizer, MDI/S, and dry powder inhalers.7 These last 2 articles claimed to be systematic reviews, although they do not clearly state their search methodology.
Researchers used a wide variety of spacers in all aforementioned studies; accordingly, one cannot be recommended as superior to others. The degree of teaching given to parents and children about MDI/S use was not described in any of the trials.
FIGURE
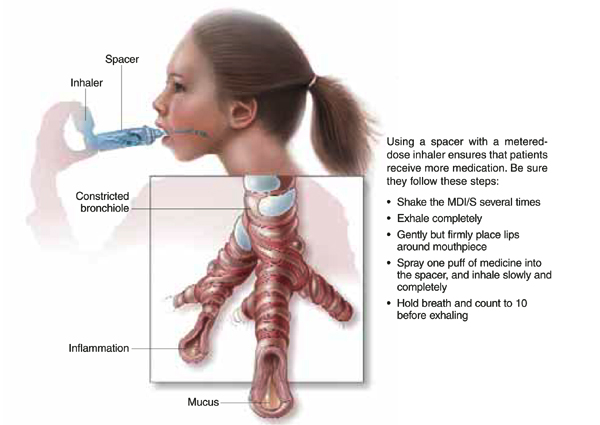
MDI with spacer is beneficial when used properly
Recommendations from others
Guidelines from the Global Health Initiative for Asthma, a collaboration of the National Heart, Lung and Blood Institute and the World Health Organization, recommend MDI/S for children with asthma due to increased efficacy and decreased cost (revised in 2002). Specifically, they recommend a spacer with a face mask for infants and preschool children, a mouthpiece and spacer for children aged 4 to 6 years, and a dry powder inhaler or breath-activated device from age 6 onwards.8 Cincinnati Children’s Hospital’s evidence-based guidelines from 1998 also recommend MDI/S for children aged >1 year with acute asthma exacerbations.9 This guideline suggests using 4 to 8 puffs from a 90 μg albuterol MDI at 1- to 2-minute intervals every 20 minutes for 1 hour, then every 1 to 4 hours subsequently.
CLINICAL COMMENTARY
Use MDIs with spacers in all but the youngest patients
Grant Hoekzema, MD
Mercy Family Medicine Residency, St. Louis, Mo
Until recently, using a nebulizer for the wheezing child or infant seemed intuitively to be the most effective way to deliver bronchodilators. However, with recent data showing that MDIs with spacers are just as effective, I have been using MDIs with spacers for all but my youngest patients. Parents as well as physicians may need to be convinced that using less technology in this case is better for their child. In some cases, parental acceptance of therapy necessitates using a nebulizer.