A 57-year-old man was referred by his general practitioner to our surgical team as an emergency admission. The patient had a 4-month history of post-prandial nausea and vomiting, occasional heartburn, and a change in bowel habits. (His normal bowel habit was 3 times a day, but it had changed to once every 2 to 5 days.) Over the past 2 months, he had lost 16 kg (35.3 lb).
His past medical history included esophagitis, peripheral vascular disease, and an inguinal hernia repair. He was a self-employed baker, a smoker of 8 pack-years, and his alcohol intake was 6.9 oz per week. There was nothing significant about his family history. His regular medications included omeprazole, simvastatin, and aspirin.
On examination, we noted bilateral fingernail clubbing, but no peripheral lymphadenopathy. His abdominal examination revealed mild, left upper quadrant tenderness.
His significant laboratory results were:
- hemoglobin, 11.6 g/dL
- mean corpuscular volume, 93.0 fL
- ferritin, 17 mcg/L
- serum folate, 2.3 mcg/L
- albumin, 29 g/L
- potassium, 3.3 mmol/L
- urea, 13.2 mmol/L with normal creatinine
- sodium, 141 mmol/L
A barium meal test showed a large food residue in the stomach, a markedly dilated duodenal loop, and a stricture at the duodenal-jejunal flexure. Computed tomography scan showed 2 simple liver cysts. Esophagogastroduodenoscopy showed moderate reflux esophagitis, a large residue of food and fluid in the stomach, and a stricture that appeared to be malignant at the duodenal-jejunal flexure.
Biopsies revealed severe, high-grade dysplasia and a possible invasive tumor. Incidentally, one of the biopsies also showed evidence of celiac disease (FIGURE 1A). The patient was started on total parenteral nutrition in light of his significant weight loss. He was transferred to surgical care and underwent laparotomy and resection of a proximal jejunal tumor.
Chemotherapy and a gluten-free diet
Final histopathology revealed a jejunal adenocarcinoma with extension to the serosal surface of the bowel (FIGURE 1B) and celiac lymph node involvement. Histology of the surgical specimen also confirmed the diagnosis of underlying celiac disease. The patient underwent adjuvant chemotherapy and was put on a gluten-free diet.
The patient began to gain weight. On a follow-up visit, he was 20 kg (44.1 lb) heavier than his presurgery weight. He was moving his bowel once a day with formed brown stool.
FIGURE 1
Duodenal biopsy revealed celiac disease and adenocarcinoma
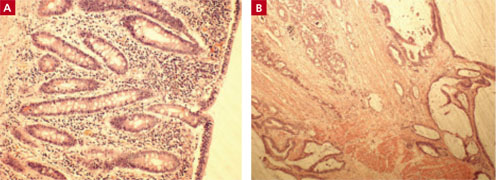
One of the patient’s biopsies showed evidence of celiac disease (A). Another revealed a jejunal adenocarcinoma (B) with extension to the serosal surface of the bowel and celiac lymph node involvement.
Anemic for years, but no one dug deeper
A detailed history revealed that the patient had been anemic since the age of 20, had always had difficulty maintaining his weight, and had been having bowel movements 3 to 4 times a day throughout his life. It was unclear why his condition was never properly investigated.
Progress was short lived
Unfortunately, while receiving adjuvant chemotherapy, our patient developed a gastric outlet obstruction that required further surgery and a palliative gastroenterostomy. Despite good palliation, the patient died several months later from progressive cancer.
A valuable reminder for us all
Celiac disease is not an uncommon cause of malabsorption of 1 or more nutrients in Caucasians—especially those of European decent.1-4 Colon cancer, gastric cancer, and celiac disease are the most important gastrointestinal causes of iron deficiency anemia.5
The seroprevalence of celiac disease is as high as approximately 1% in North America and Western Europe, with a high ratio of un-diagnosed to diagnosed cases.4,6-8 The most serious complication of celiac disease is the development of a malignancy.1,9-12 Incidence of both gastrointestinal and nongastrointestinal neoplasms (as well as intestinal lymphoma) is higher in patients with celiac disease.1,9-11,13 Small-bowel lymphoma appears to be significantly associated with unrecognized celiac disease.7
Data from various studies suggest a protective role for a gluten-free diet against malignancy in celiac disease and give further support for advising all patients to adhere to a strict gluten-free diet.9,10,13,14
Follow the clues: Nutrient deficiencies, including folate and iron deficiency anemia—with all of their associated signs and symptoms—are not disease entities, but clues to diseases. We must remain vigilant in our investigative efforts.
CORRESPONDENCE Arash Assadsangabi, MD, Gastroenterology Department, Bristol Royal Infirmary, Marlborough Street, Bristol, BS2 8HW, UK; arash.sangabi@gmail.com