Practice recommendations
- Talk to every male patient over the age of 50 about urinary function (C).
- Utilize questionnaires, such as the International Prostate Symptom Score to evaluate the patient's perception of symptom severity and quality of life (A).
- Rule out potential causes of lower urinary tract symptoms with a thorough medical history, focused physical exam (including digital rectal examination and neurological assessments), and appropriate laboratory evaluations (C).
- When choosing treatment for benign prostatic hyperplasia, remember that quality of life is generally more important than symptom severity (A).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
"My wife is mad at me—and she's worried, too," says Dan, a 65-year-old patient of yours. "She's been telling me to come see you, but I've been putting it off.
"I've been getting up 4 and 5 times a night to urinate, and we can't drive an hour without me having to stop at least once to use a restroom."
With a deep sigh, Dan says: "My wife is worried that I have cancer or something."
"And I'm worried, too," he admits.
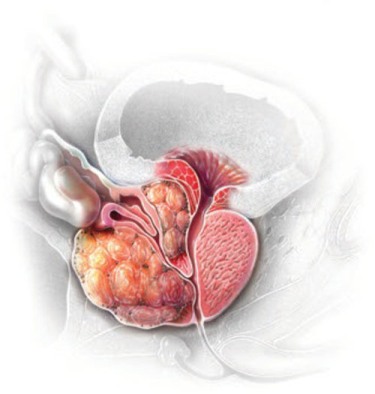
Benign prostatic hyperplasia (BPH), and its clinical expression as lower urinary tract symptoms—urinary frequency, urgency, nocturia, decreased force of stream, and incomplete bladder emptying—comprise a major health concern for many older men. Approximately 50% of men over age 60 have at least microscopic BPH, while 90% over age 90 have evidence of the abnormality.1
Many men fail to seek help for lower urinary tract symptoms associated with BPH,2-4 even though these often moderate to severe symptoms are associated with decreased quality of life, anxiety, and depression.5 Your patient may be uncomfortable broaching the subject, as Dan was, for fear that he may have cancer. He may dismiss the symptoms as a natural consequence of aging,6 or he may believe that there are no effective treatments or that treatment will cause unwanted side effects.
Bring up the subject with all men over 50
To dispel these misconceptions and ensure that there are no current or ensuing serious complications,4 you should routinely talk about urinary function with every male patient over age 50. Because the incidence of BPH increases not only with age but also with other comorbid conditions such as diabetes7 and erectile dysfunction (ED),8 you should discuss the symptoms and potential complications of BPH with patients who present with these comorbidities. You can reassure them that BPH is not cancer, nor is it a precursor to prostate cancer; rather it is a fairly common, treatable disorder.
What's right for your patient? Watchful waiting? a-Blocker therapy? Surgery?
Questionnaire can help, addresses quality of life
Questionnaires such as the International Prostate Symptom Score (IPSS) (PATIENT HANDOUT)9 and the similar American Urological Association symptom index (AUA-SI) (available on page 44 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf) can help you evaluate your patient's symptom severity.2,6
The IPSS, with 3 categories of symptom severity (mild 0 to 7, moderate 8 to 19, severe 20 to 35) and a global quality-of-life question also referred to as the "Bother Score," is a validated tool for monitoring disease distress and clinical change.10,11 The quality-of-life question is a good indicator for assessing whether watchful waiting might be preferred to active treatment.9,12
Further categorizing the symptoms is not helpful. Lower urinary tract symptoms have traditionally been divided into irritative symptoms such as nocturia, urgency, and frequency, attributed to bladder and prostatic smooth muscle contractions, and obstructive symptoms such as hesitancy, decreased force of stream, and incomplete emptying, attributed to increased glandular mass.1 This distinction, however, is not helpful inasmuch as irritative symptoms can result from increased tissue mass alone and obstructive symptoms from muscle hypertonicity alone; additionally, most BPH patients have a combination of both.13,14
Consider comorbidities and overactive bladder
Common comorbidities for a patient with BPH include obesity, diabetes mellitus, and low high-density lipoprotein levels. Both irritative and obstructive symptoms are likely, without prior lower urinary tract disorders or ongoing neurological disease.13-15 Multiple epidemiological studies have established clear, clinically relevant associations between BPH-related lower urinary tract symptoms and ED and ejaculatory dysfunction.8
It is also important to note that lower urinary tract symptoms may often arise due to overactive bladder; in fact, symptoms of overactive bladder and BPH overlap to a large degree.16 The diagnostic challenge is only increased by the fact that while overactive bladder is an additional cause of lower urinary tract symptoms, it may also coexist with BPH-related bladder outlet obstruction.17 The similarity in clinical presentation of the 2 conditions may make them hard to distinguish.