Jeremy T. Reed, MD, MPH & TM Colin M. Grant, DO Carl R. Darnall Army Medical Center, Fort Hood, Tex jeremy.t.reed8.mil@mail.mil
DEPARTMENT EDITOR Richard P. Usatine, MD University of Texas Health Science Center at San Antonio
The authors reported no potential conflict of interest relevant to this article.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the US Army Medical Department or the US Army at large.
Our patient’s tongue mass hadn’t bothered her until she became pregnant; that’s when it got larger and caused problems swallowing and breathing. A simple test confirmed our suspicions.
A 26-year-old nonsmoking obese woman presented to our primary care clinic for treatment of a mass at the back of her tongue that was causing intermittent dysphagia and nocturnal choking when she was lying down. She had first noticed the mass 3 years ago; it had been asymptomatic until her recent pregnancy, when its size increased significantly. She denied hemoptysis and dyspnea.
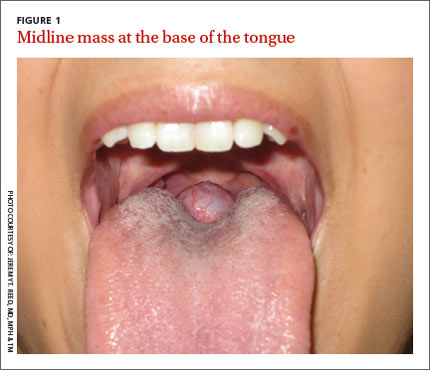
On examination, we noted a purplish, 3 × 3 cm, midline posterior tongue mass with marked superficial vasculature (FIGURE 1). The mass was firm, nontender, and non-friable on palpation. Nasopharyngoscopy revealed a patent airway. There were no other lesions.
WHAT IS YOUR DIAGNOSIS? HOW WOULD YOU TREAT THIS PATIENT?