Robyn M. Marszalek, MD Yoon-Soo Cindy Bae-Harboe, MD Meera Mahalingam, MBBS, PhD Katherine Masterpol, MD Boston University School of Medicine, Mass; Boston Medical Center, Mass (Drs. Marszalek and Bae-Harboe); Skin Pathology Laboratory, Boston, Mass (Dr. Mahalingam); Dermatology Associates of Winchester, Mass (Dr. Masterpol) drkasia@gmail.com
DEPARTMENT EDITOR Richard P. Usatine, MD University of Texas Health Science Center at San Antonio
The authors reported no potential conflict of interest relevant to this article.
The asymptomatic lesion on our HIV-positive patient’s penis suggested an STD, but the patient said he hadn’t had any sexual partners for many years.
A 36-year-old man sought treatment at our outpatient dermatology clinic for an asymptomatic penile lesion that he’d had for a month. He’d been diagnosed with human immunodeficiency virus (HIV) infection 5 years earlier, and was taking highly active antiretroviral therapy of emtricitabine 200 mg/tenofovir 300 mg daily and nevirapine 200 mg twice a day. The patient’s CD4 T-cell count was 530 cells/mm3 (normal for a nonimmunocompromised adult is 500-1200 cells/mm3) and his viral load was undetectable. He wasn’t in a committed relationship and reported having no sexual partners for many years.
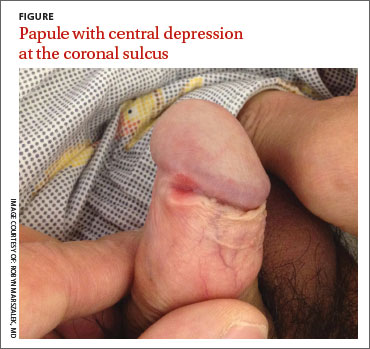
Physical examination revealed an indurated, 7 mm white to pink keratotic papule with a central depression near the coronal sulcus (FIGURE). No ulcers or erosions were seen. The patient denied having urethral discharge, pain, or pruritus. During the previous week, he said he’d applied triamcinolone cream 0.1% twice daily to the area with no improvement.
WHAT IS YOUR DIAGNOSIS? HOW WOULD YOU TREAT THIS PATIENT?