ANSWER
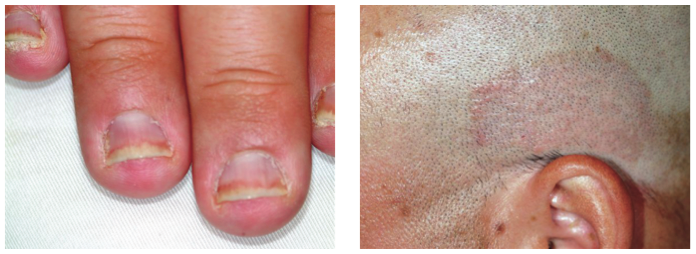
The correct answer is psoriasis (choice “d”), which often involves nail and skin changes such as those seen in this case. There was no particular reason to think this patient had an infection of any kind, but, as is often the case, the original provider considered only one diagnostic possibility.
DISCUSSION
Nail disease can be problematic for both patient and provider. Arguably the biggest issue with it, initially, is “the one-item differential”—the idea that all nail disease can be classified as “fungal infection” simply because neither the patient nor the provider considers any other explanation for the changes seen. This case illustrates that dilemma nicely.
Psoriasis affects more than 2% of the US population, making it a common skin disorder. As this case illustrates, it may affect several areas with diverse but predictable morphologic presentations, all appearing at the same time.
The key diagnostic points from this case include:
• Stress is a known trigger for psoriasis vulgaris.
• The patient’s nails failed to respond to terbinafine treatment.
• There was no obvious source of fungal infection (eg, contact with animals) or reason for him to have a yeast infection (eg, diabetes) or develop mold “infection” in the nails (eg, trauma from digging in soil).
• Fungal infections are about 18 times less likely to occur in the fingernails than in the toenails.
• A unifying explanation for simultaneous nail and skin changes was needed.
• The nail and skin changes seen here are quite typical for psoriasis.
Most important, though, is the need to overcome the urge to hop on the “fungal bandwagon” by first considering other diagnostic possibilities.
Continue for the treatment of this condition >>