MAKING THE DIAGNOSIS Presenting behaviors Symptoms of ADHD typically manifest in academic settings. The greater frequency of ADHD diagnosis and treatment in boys may derive from differences in how the genders externalize behaviors.19 While boys often exhibit more impulsive and aggressive behavior, girls internalize symptoms and are more likely to be inattentive. As a result, girls are less likely to be disruptive in the classroom and may not be referred for evaluation. Boys, on the other hand, may be overdiagnosed due to their disruptive behaviors.19 Daley indicates that inattention (eg, daydreaming) and hyperactivity (eg, fidgeting) symptoms become more apparent in structured settings, such as a classroom.15
Any child who requires a mental health assessment should also be screened for ADHD; if the results of the screening suggest ADHD, a full evaluation is warranted.20
Diagnostic criteria According to the American Psychiatric Association’s criteria—outlined in the Diagnostic and Statistical Manual of Mental Disorders–IV (Text Revision) (DSM-IV-TR) and the subsequent DSM-5—the diagnosis of ADHD requires that the patient have at least six symptoms of inattention, hyperactivity, and/or impulsivity.4,21,22 For patients ages 17 or older, the DSM-5 requires five symptoms of inattention or hyperactivity-impulsivity.21
Children are usually unable to complete one task prior to starting another and are easily distracted by noises otherwise ignored by others (eg, lawnmowing, background conversation).4 They may also exhibit excessive fidgeting and interrupt formal conversations or lectures.4 Inappropriate behavior relative to the child’s developmental level must have been present for at least six months prior to age 7 (according to DSM-IV-TR)4 or age 12 (DSM-5).21
In addition to exhibiting the above symptoms for a minimum of six months, impairment must be observed in at least two settings (home, school, or work), with obvious clinical impairment in social, academic, or occupational functioning.4 ADHD symptoms can vary depending on the setting; the child may have more difficulty paying attention and following directions in a classroom filled with children than in an environment with less stimuli (eg, one-on-one home situations).11
Children who exhibit ADHD symptoms in only one setting may actually have problems secondary to cognition, emotional maturity, or feelings of well-being in a particular setting.11 Therefore, the clinician must rely on multiple sources of information (eg, parents, teachers, other caregivers) in order to make the diagnosis of ADHD.23 A teacher should have had regular contact with the child for at least four to six months in order to provide an accurate evaluation of symptoms and their persistence.5
Assessment scales Validated parent and teacher instruments, along with the DSM-IV-TR criteria, can be used to obtain data to support a diagnosis of ADHD.5,24
The Conners Comprehensive Behavior Rating Scales and the ADHD Rating Scale IV (DSM-IV) can be used by teachers and parents to document behaviors of preschool-aged children.5
The Vanderbilt Assessment Scales, which have been validated in both primary care and referral settings, may be used for children older than 4.5
In addition to parent- or teacher-reported data, further evidence of functional impairment may be gleaned through a review of report cards, standardized testing, and school records (eg, attendance or disciplinary actions).24
Differential diagnosis The differential diagnosis should include other mental health conditions, sleep disorders, and any possible underlying medical or developmental problems.24 Hyperthyroidism and lead toxicity, as examples, could elicit symptoms consistent with ADHD.11 When the diagnosis is in doubt, coexisting conditions are present, or treatment options are in question, the primary care clinician should refer the patient to a pediatric or mental health specialist for further evaluation.23
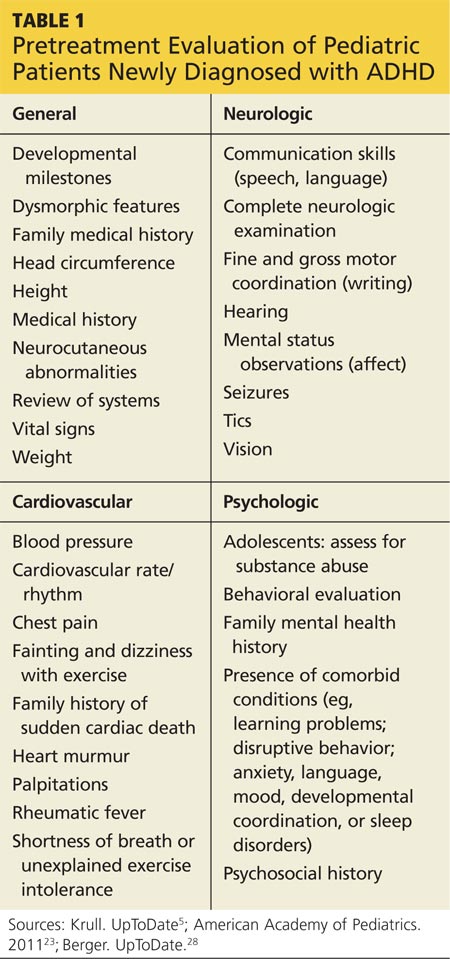
BEFORE TREATMENT After the diagnosis is made but before treatment commences, a complete review of systems, physical and psychologic evaluation, cardiac and sleep history, thorough family history pertaining to mental health and medical conditions, and an age-appropriate interview are required.24 The exam results assist in identifying other concerns that would indicate the need for appropriate diagnostic testing and/or referral (see Table 1).
Although stimulant treatment for ADHD has not been shown to increase cardiovascular events in otherwise healthy young people,25 experts differ in their opinions about the need for screening ECG prior to treatment initiation. The American Heart Association recommends a screening ECG before stimulant therapy is initiated,26 while the American Academy of Pediatrics (AAP) does not, as long as the history and exam results yield no cardiac findings.27 Since the Prescribing Information for most ADHD medications cautions against use in patients with known serious cardiac abnormalities, if exam findings suggest the possibility of cardiovascular disease, further evaluation with ECG and referral to a pediatric cardiologist are indicated.26,28
In the interview, the clinician should explore the patient’s perception of his or her behavior in response to family and social relationships and academic performance (eg, parent-teacher communication, report cards, detentions, suspensions). The psychosocial history may provide an explanation for acute onset of symptoms or coexisting disorders. Family history provides valuable insight regarding the health and cognitive abilities of family members, as well as the possibility of genetic influences on the child.24
Parents should be advised that ADHD is a chronic condition that requires a long-term treatment approach for symptoms that may last into adulthood. Identification of goals and treatment success depend on collaborative efforts with parents, teachers, clinicians, caregivers, and mental health clinicians.24