MEDICATION RECOMMENDATIONS AAP medication recommendations are age-specific and should be used only if the patient meets DSM-IV-TR criteria.24 An overview of both stimulant and nonstimulant treatment options for ADHD is provided in the Figure.
When an ADHD treatment regimen does not result in improved symptoms and functioning, the clinician should revisit the treatment plan and differential diagnosis. After reevaluation, the clinician may choose to add or change medication type or dose, adjust behavioral therapy, or consider the possibility of language or learning disabilities, mental health disorders, other psychosocial stressors, or poor adherence to the treatment plan.24
Parents may refuse stimulant therapy for their child, fearing future drug use (or abuse) in adolescence.24 Clinicians should respect parents’ decisions to defer stimulant therapy, while at the same time clarifying concerns or misunderstandings in order to provide optimal care for the child.24 Studies have demonstrated that stimulant treatment for ADHD has a protective effect, with outcomes suggesting significantly decreased risk for drug or alcohol dependence.36
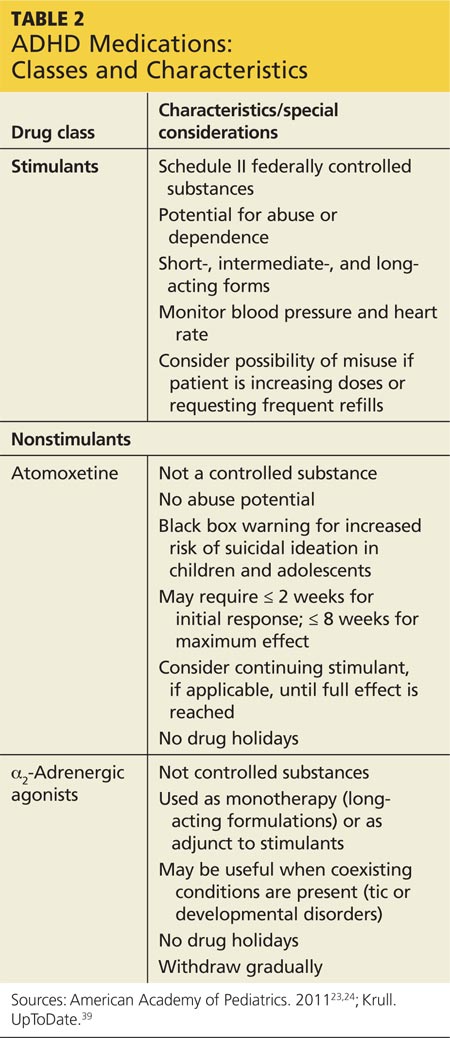
Clinician-provided anticipatory education about dose titration, expected treatment results, and potential adverse effects will help prepare parents for the ADHD medication management process.23 The length of time needed for dose titration varies by class of ADHD medication (see Table 2). For stimulants, effects on core symptoms may be seen within the first week. Nonstimulants take longer: up to six weeks for atomoxetine and up to four weeks for the a2-adrenergic agonists.24
Stimulants Evidence strongly supports stimulants as first-line treatment for ADHD in children ages 6 and older.23 Stimulants are safe and efficacious in reducing the core symptoms of inattention, hyperactivity, and impulsivity.23 The initial choice of stimulant depends on the individual child’s needs. It should be noted that, although decreased growth rates have been observed in children taking stimulants, this effect ends by the third year of treatment.38 If maximum doses are reached and desired effects are not achieved with the first stimulant, choosing an alternate drug in the stimulant class may be an effective option.24 Clinicians may also consider other drug classes based on the comprehensive exam, adverse effects profile, contraindications, and individual responses.
Nonstimulants Nonstimulant medications include atomoxetine and the a2-adrenergic agonists extended-release clonidine and extended-release guanfacine.24
Atomoxetine. Atomoxetine is a selective norepinephrine-reuptake inhibitor that may be prescribed if substance abuse or diversion is suspected or if stimulant therapy is contraindicated, undesirable, or unsuccessful.24,39 Using weight-based dosing for titration,37 the first week of therapy should begin with a half-dose to minimize sedation or gastrointestinal symptoms.24 While atomoxetine can be quite effective, caution should be used when prescribing this agent, as it carries a black box warning for suicidal ideation.24
α2-Adrenergic agonists. Both extended-release clonidine and extended-release guanfacine are α2-adrenergic agonists that may be beneficial when stimulants and atomoxetine have failed or when there are coexisting conditions.37 Either clonidine or guanfacine can be given in combination with a stimulant, if stimulant or atomoxetine treatment alone is unsuccessful or if adverse effects are unacceptable.24,39 Sedative effects and withdrawal irritability are more common with clonidine than with guanfacine, and when discontinued, these medications should be tapered to avoid blood pressure changes.24,40
Age-specific recommendations Medications should be selected based on age ranges. In preschool-age children (ages 4 to 5), methylphenidate is recommended when target behaviors and impaired functioning persist for nine months in both home and day care/school settings, despite behavioral therapy.23,24 As examples, medication may be warranted if the child poses a significant risk of injury to other children or caregivers and/or faces expulsion from preschool or day care because of his or her behaviors.34
Risks and benefits should be considered carefully before medical therapy is initiated in this group. Further, the lowest possible starting dose of methylphenidate is preferred for preschoolers due to their slower metabolism.24 While dextroamphetamine is FDA approved for children younger than 6, efficacy and safety have not been proven in this age group and the AAP does not recommend it.23
For children ages 6 to 18, the AAP recommends combined treatment with medication and evidence-based behavioral training for the patient, parent, and teacher. In the adolescent population, evidence supports use of stimulants as first-line therapy, but with close monitoring for medication misuse.23 Misuse may become apparent through increased prescription refills; if identified, ADHD medication should be discontinued and substance abuse treatment initiated before ADHD therapy recommences.24